


INTRODUCTION
Since people are living longer and keeping their teeth longer, we need to be able to deal with the endodontic implications, and this includes treating an increasing number of calcified root canals. It would be a shame to recommend extraction of a perfectly functional and restoratively sound tooth because of concern over, or the inability to manage, calcified roots.1
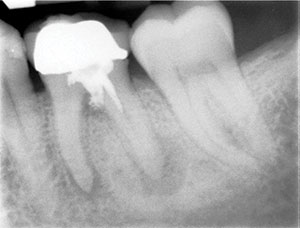
Once calcified canals are identified radiographically (Figure 1), the clinician should keep in mind the following fundamental protocols pertaining to instrumentation: locating the canals with proper magnification; instrumenting with stiff, pre-curved stainless steel hand files, followed by narrow and flexible mechanized NiTi files; and, all the while, ensuring the canals are kept lubricated during the filing process. In turn, instrumenting calcified canals comes down to having the proper armamentaria and techniques (Table 1).
ENHANCED MAGNIFICATION
If you can’t see it, you can’t treat it. So, before instrumenting a calcified canal, you need to locate it within the endodontic access. For this, enhanced magnification and illumination is an absolute must. This could be in the form of dental loupes with a bright LED headlight (eg, Designs for Vision, SurgiTel, or Orascoptic) (Figure 2) or, better yet, a dental operating microscope (ie, ZEISS or Global Surgical) (Figures 3 and 4). A case in point is the clear benefit of magnification in locating the often calcified MB2 canals of maxillary molars.2
 |
| Figure 1. Calcified canals identified in the mesial root of tooth No. 30. |
 |
 |
 |
| Figures 2 to 4. Visualization is enhanced with the use of loupes and microscopes. (Figure 2) Dental loupes with headlight (Designs for Vision) and dental operating microscopes from (Figure 3) ZEISS and (Figure 4) Global Surgical. |
Without sufficient visualization and illumination into that little endodontic access, the clinician will likely be spending too much time looking for a calcified canal and/or may not be able to locate it at all (Figure 5). Worse yet, you’ll be more likely to perforate the tooth in the process of drilling and looking for a canal that may be the size of a strand of silk, so to speak (Figure 6).
INSTRUMENTATION
Once any calcified canals are identified, one needs to have the right files to negotiate them, and this would include both stainless steel (SS) hand files and NiTi mechanized files (rotary and/or reciprocating).3
Hand Instrumentation
A fundamental aspect of instrumenting that has not changed over the years is the need to begin all canal instrumentations with small stainless steel hand files.4 No matter what special and popular small and flexible NiTi files come to market, there is absolutely no substitute for SS hand files in initial instrumentation.5 The small hand files are important in creating a “glide path.”6 This is the initial canal preparation that extends from the orifice to the apex, which the proceeding files are meant to follow.
 |
| Figure 5. A view of MB1, MB2, and DB canals in a maxillary molar at 15x magnification. |
 |
 |
| Figure 6. An endodontic mishap in tooth No. 30. The pulp floor was perforated during the process of looking for calcified mesial canals. | Figure 7. Pre-curved #8 and #10 stainless steel hand files. |
 |
 |
| Figures 8 and 9. An instrumentation mishap in a calcified root. (Figure 8) Preoperative view of tooth No. 3 with a calcified and curved MB root. (Figure 9) A separated file in a calcified and curved MB2 of tooth No. 3 that was not managed properly. |
 |
 |
| Figures 10 and 11. Proper management of calcified MB and DB roots in tooth No. 14. (Figure 10) Pre-op view of tooth No. 14, showing canal calcifications. (Figure 11) Postoperative view of tooth No. 14 with 4 canals treated to length and canal curvatures maintained. |
It is important to note that nearly all canals have some curvature, regardless of what they look like in a 2-D radiograph. With this in mind, it is important to pre-curve all your small SS files (Figure 7) and to work them in a “watch-winding” fashion.5 This is your best and safest way to negotiate canals and prevent ledging, zipping, or apical blockage. (Note: zipping is the result of the tendency of an instrument to straighten inside a curved root canal, resulting in over-enlargement of the canal.) The practice of pre-curving and watch winding the SS hand files is possibly the most important part of managing canals, let alone calcified canals. If you do not do this correctly, you may easily create a tiny apical ledge or block that will only get worse once you use larger SS hand files or mechanized NiTi files. In addition, you may easily lose your apical patency in the process.7,8
When trying to manage a calcified canal, the use of very small SS hand files, such as .06, .08, and .10 files, is often a must. However, traditional SS K-files of these sizes will most likely not be able to negotiate calcified and curved canals. They tend to easily unwind, buckle, or—worse yet—fracture. While we worry about NiTi file separation, we must remember that SS files can also separate, especially in tight canals. So I strongly recommend the use of stiff hand files, such as C-files (Dentsply Sirona Endodontics) or EndoSequence Stiff K-Files (Brasseler USA). Consider a #6 hand file that is .06 in diameter but is about as stiff as a traditional .08 or .10 SS hand file. That is how C-files are characterized.
The importance of SS files in the management of calcified canals cannot be overstressed. If your hand file does not go to length, then please do not attempt to instrument to length with any NiTi file9 (Figures 8 and 9).
 |
 |
 |
 |
| Figures 12 to 15. These NiTi files are tailored for the management of calcified canals and to produce a glide path: (Figure 12) XPlorer (Clinical Research/CLINICIAN’S CHOICE Dental Products) NiTi rotary files, (Figure 13) ESX Scout (Brasseler USA) NiTi rotary files, (Figure 14) Pathfiles (Dentsply Sirona) NiTi rotary files, and (Figure 15) a WaveOne Gold Glider (Dentsply Sirona) NiTi reciprocating file (pre-curved). |
Mechanized Instrumentation
Companies are well aware of the demographics that include an increasing number of elderly patients with a greater number of cases that require the successful management of calcified canals (Figures 10 and 11). In turn, with improved metallurgy and engineering, endodontic manufacturers have recently introduced NiTi endodontic files that are specifically designed to manage calcified canals and create or enhance glide paths.10 These files are able to do what SS files attempt to do, but these instruments do it better and more efficiently.11 This new generation of narrow and flexible NiTi mechanized files has been shown to follow natural canal curvatures better than hand SS files.4,11 One must remember that the larger the SS file used in a curved canal, the more likely it is to transport, zipp, or even block a canal that it cannot easily negotiate. This is because SS hand files lack the flexibility to negotiate canals and don’t have the design to cut dentin/walls less aggressively.1
The following are examples of narrow and flexible NiTi files:
- XPlorer (Clinical Research/CLINICIAN’S CHOICE Dental Products): This is one of the first glide path NiTi files to come to market (Figure 12). These files are available in .01 and .02 tapers (the same narrow taper as SS hand files). These rotary NiTi files bring the benefits of flexibility and very narrow tapers.
- ESX Scout (Brasseler USA): These are rotary NiTi files, size .15 at the tip, available in .02 and .04 tapers, and are also meant to provide the initial NiTi negotiating and shaping of a canal (Figure 13).
- Pathfiles (Dentsply Sirona Endodontics): These narrow (.02 taper) and flexible NiTi files come in 3 sizes (.13, .16, and .19) (Figure 14). The increase in file sizes (from .13 to .16 to .19) makes it easier to go up in file size versus standard ISO file sizes. This is due to a consistent increase in diameter from one Pathfile to another.
- WaveOne Gold Glider (Dentsply Sirona Endodontics): This is one of the newest glide path NiTi files on the market (Figure 15). This file may be considered the culmination of the latest in metallurgy and reciprocating instrumentation. They are size .15 and .02 taper at the tip and have an increasing taper coronally. The file can be pre-curved, which may be helpful in accessing posterior teeth. Studies have shown the benefits of reciprocation, such as that of WaveOne, when it comes to fracture resistance and the ability to follow canal curvatures compared to traditional rotary NiTi filing.7,12
CANAL LUBRICATION
This may sound obvious, but make sure to never instrument in dry canals. As we focus on tiny canals, we may forget to keep them lubricated. Forgetting to do so will increase the chance of file separation or apical blockage.4 So, please lubricate and re-lubricate the canals throughout the procedure.1 RC-Prep (Premier Dental Products) has been a popular lubricant for many years. However, if this is to your liking, you may also want to consider something that works like RC-Prep but has EDTA to help remove the smear layer (such as ProLube [Dentsply Sirona Endodontics]). Some clinicians may opt to use 17% EDTA as a lubricant in calcified canals. Others simply use sodium hypochlorite as a lubricant because it provides all-in-one lubrication, antibacterial, and tissue-dissolving properties.13
Note that no lubricant will miraculously flow into a calcified canal and “soften” or “open” the canal to make instrumentation easier. What you end up using may depend more on how things handle in your hands. I, for one, do not like using RC-Prep (or other similar lubricants), as file handling can be difficult and slippery if these materials get onto your fingers. Furthermore, they lack the antibacterial and tissue-dissolving properties of sodium hypochlorite. Again, no matter what you use, the key is to make sure you never use the instrument in dry canals.
 |
CLOSING COMMENTS
Having discussed initial canal preparation, it is not as important to review the main NiTi filing systems that will still need to be used to complete the instrumentation. That is because once you have successfully achieved a good glide path with hand SS files and NiTi mechanized files, the rest becomes a lot easier and should be considered like filing a regular-sized canal. Of course, you should use a NiTi file system that is fracture resistant and can follow canal curvatures well.
I would emphasize the need to always know your limits. Even with the proper armamentaria and protocols, you may still find it difficult to manage some calcified canals. There is nothing wrong with stopping mid-treatment in a calcified tooth if you realize it may still be too complex for you. The key is to know when to stop and refer to an endodontist. If you try instrumenting too much while getting nowhere, you may do more harm than good by worsening a ledge, zipp, or apical block.
Finally, in an aging population, the need to manage calcified canals is increasingly important. Thanks to enhanced magnification and instrumentation, doing so is now easier and safer than ever before. Having the proper armamentaria and following fundamental clinical protocols is crucial when instrumenting calcified canals.
References
- Hargreaves KM, Berman LH, eds. Cohen’s Pathways of the Pulp. 11th ed. St. Louis, MO: Elsevier; 2016:209-279, 324-386.
- Schwarze T, Baethge C, Stecher T, et al. Identification of second canals in the mesiobuccal root of maxillary first and second molars using magnifying loupes or an operating microscope. Aust Endod J. 2002;28:57-60.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod. 2004;30:559-567.
- Patiño PV, Biedma BM, Líebana CR, et al. The influence of a manual glide path on the separation rate of NiTi rotary instruments. J Endod. 2005;31:114-116.
- Mounce R. Endodontic K-files: invaluable endangered species or ready for the Smithsonian? Dent Today. 2005;24:102-104.
- Dhingra A. Glide path in endodontics. Endodontology. 2014;26:217-222.
- Dhingra A, Nagar N, Sapra V. Influence of the glide path on various parameters of root canal prepared with WaveOne reciprocating file using cone beam computed tomography. Dent Res J (Isfahan). 2015;12:534-540.
- Franco V, Tosco E. The endodontic line: a clinical approach. G Ital Endod. 2013;27:2-12.
- Mullaney TP. Instrumentation of finely curved canals. Dent Clin North Am. 1979;23:575-592.
- van der Vyver P. Creating a glide path for rotary NiTi instruments: part one. International Dentistry. 2011;13:14-25.
- West J. Manual versus mechanical endodontic glide path. Dent Today. 2011;30:136-140.
- Ahn SY, Kim HC, Kim E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: a systematic review of in vitro studies. J Endod. 2016;42:1009-1017.
- Iqbal A. Antimicrobial irrigants in the endodontic therapy. Int J Health Sci (Qassim). 2012;6:186-192.
Dr. Haas is a certified specialist in endodontics. He maintains a full-time private practice limited to endodontics and microsurgery in Toronto. In addition to being an international lecturer, Dr. Haas is also a Fellow of the Royal College of Dentists of Canada and is on staff at the University of Toronto Faculty of Dentistry and the Hospital for Sick Children. He can be reached by visiting haasendoeducation.com.
Disclosure: Dr. Haas reports no disclosures.
Related Articles
Questions to Ask Prior to Root Canal Treatment








