
INTRODUCTION
What constitutes a beautiful smile? There are a number of criteria that are viewed as essential components of an attractive smile. The lips frame the smile, so we as dentists must balance what is seen in the interaction between the teeth and the lips.1 The analysis of the teeth is broken down into micro- and macro-aesthetic components. Micro-aesthetics concern how an individual tooth looks with respect to internal color, shape, positions of the line angles, and how the tooth looks in respect to the adjacent teeth. Macro-aesthetics encompass those characteristics that are seen from a distance: How much tooth or incisal display is revealed? What is the color and shape of all the teeth in relation to the upper and lower lip? Does the smile fill the buccal corridor? Are the teeth angled in the correct orientation? What are the shapes of the incisal embrasures, and how is the gingiva framing the teeth?2
The discussion in this article will concentrate on a case study related to the macro-aesthetic elements of a smile.
ESTABLISHING BEAUTY: MACRO-AESTHETIC CRITERIA
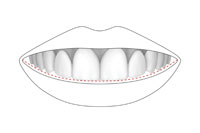
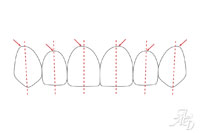
Among the many criteria of beauty, the incisal plane and dental midline play a role in this perception. In the ideal smile, the midline of the teeth would match the midline of the face. The interproximal contact area of the central incisors would be perpendicular to the horizon, a horizontal line parallel to the ground. The contact area of the anterior teeth are in a progression from the largest contact area between the central incisors, to a slighter contact between the laterals and cuspid.3 In this ideal smile, the incisal plane would be perfectly horizontal, follow the lower lip-line, and would bisect the angle formed from a line from nasion to cupid’s bow, continuing down through the contact area of the maxillary central incisors (Figures 1 and 2).4
 |
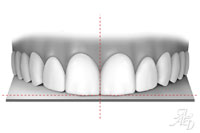 |
| Figure 1. The ideal incisal edge follows the lower lip-line. | Figure 2. The incisal plane is perpendicular to the dental midline. |
Macro-aesthetic variations would be most evident when you first see someone’s smile. Differences from an ideal (“perfect”) smile become more visible as any defect becomes more pronounced. One such area of deviation relates to a perfectly level line of the maxillary incisal edges. Related to this is the contact area of the central incisors. A study by Kokich, et al5 has been done that analyzes the amount of deviation from the midline that would be acceptable to the human eye, with evaluation done by orthodontists, general dentists, and nondental professionals. Among other characteristics of a smile, the study also determined the amount of vertical cant of the incisal plane and midline that would be noticeable. The results were: a 4-mm shift of the midline was noticeable by general dentists and laypeople, where a dentist could detect a one-mm plane asymmetry compared to a 3-mm cant by a layperson. This study shows the importance of correcting as many deficiencies of a smile when we diagnose and treat our patients.
CASE REPORT
Treatment Planning and Diagnosis
A 27-year-old female who was unhappy with her smile presented to our office. A comprehensive examination was performed,6 which included evaluation of the temporomandibular joint (TMJ), a full periodontal examination, and evaluation of the teeth with shape and color noted. A complete intraoral radiographic and photographic series was taken. Her smile was then evaluated, and it was clinically evident that she had an incisal cant that was higher on the right side than on the left. This was apparently caused by a developmental asymmetry that allowed her left condyle to grow longer than her right side. Her face, lips, and teeth were all lower on the left side (Figures 3 and 4). She had completed orthodontic treatment several years earlier, but the asymmetry was not corrected. As a result, the axial inclinations of the individual teeth were also inappropriate (Figures 5 to 7).
 |
 |
|
Figure 3. The patient’s left side lower lip is canted downward. |
Figure 4. Preoperative photo showing the canted lip and incisal plane. |
 |
 |
| Figure 5. The teeth are angled medially, with more angulation toward the posterior. | Figure 6. Preoperative retracted full-mouth view (1:2 magnification). |
 |
| Figure 7. Preoperative retracted close-up view (1:1 magnification). |
Evaluation of her TMJs was done and loading was comfortable.7 However, she had tension headaches originating from the temporal area, and she felt that she had more than one bite. Based on this information, it was decided to establish a stable occlusion first through the use of an occlusal/muscle deprogrammer. It was anticipated that the occlusion could be stabilized and treatment would be conservative in its approach, utilizing direct resin bonding in some fashion. Models were taken for the deprogrammer, sent to the dental laboratory, and then delivered a few weeks later. Once her occlusion was comfortable, diagnostic models from new impressions were fabricated. The plaster models were then mounted, using a bite registration that was tak
en with the deprogrammer in place, on a Panadent articulator (Panadent). Then a diagnostic equilibration was done. A diagnostic wax-up, which would simulate a level incisal plane, was created by our dental laboratory team (Figure 8). A putty matrix (Sil-Tech [Ivoclar Vivadent]) was molded over the wax mockup on the plaster model.
When the patient returned to the office at her next visit, a temporary BIS-GMA resin (Protemp Plus [3M ESPE]) was injected into the prefabricated putty matrix and placed into her mouth for 3 minutes. Removal of the putty matrix left the temporary resin in place over the teeth. This allowed the patient and me to view and evaluate the shape of the proposed treatment that would align her anterior teeth. The patient was very pleased, and we decided to proceed with the definitive treatment. Options of treatment included: porcelain veneers with tooth preparation; prepless veneers; and conservative direct resin bonding, which would lengthen the teeth only, leaving the rest of her anterior teeth untouched. It was anticipated that a no-preparation technique (except to lightly sand the facial surfaces with a coarse Sof-Lex [3M ESPE] disc, to aid in retention) would be used.
|
Technology Implications: Dentrix Brings “Intelligent Technology” to Its Software
|
|
Lou Shuman, DMD KEY FEATURES OF DENTRIX PRACTICE ADVISOR
In our opinion at the Pride Institute, we feel Dentrix Practice Advisor has raised the bar as an essential practice management tool to assist in engaging in critical thinking, problem solving, and most importantly, implementation. |
Minimally Invasive Lip and Perioral Treatment
Evaluation of her smile with the photos, and clinically viewing her face, demonstrated a drooping lower lip on her left side. After treatment acceptance, the use of BOTOX (Allergan) treatment was explained and discussed with the patient. I felt that a conservative single injection of 4 units of BOTOX in her left depressor anguli oris muscle may inhibit the muscle action and prevent the left side of her lip from drooping.8 She agreed to this adjunctive treatment, and BOTOX was injected. She was then scheduled to return a few weeks later to begin the minimally invasive aesthetic treatment.
Minimally Invasive Aesthetic Operative Treatment
When the patient returned to our office, the effects of the BOTOX had reduced the muscle activity as expected, giving her the appearance of a level lower lip (Figure 9). The prefabricated putty matrix that was made from the diagnostic wax-up was then sectioned, leaving only the lingual aspect, and covering the incisal edges wrapping to the facial-incisal angle (Figures 10 and 11). The facial surface of the putty matrix was removed. The incisal edges were going to be leveled through the use of direct resin bonding.
The treatment began with the central incisors. Before acid etching, the proposed colors were quickly applied to determine the correct colors that were needed. It is important to do this before the teeth dehydrate and they look too light. The putty matrix was held in place on the lingual by my assistant, and Shade OW Renamel Hybrid (Cosmedent) was applied directly against the putty matrix to act as the lingual shelf. This also established the proper incisal length. Additional hybrid colors (B-1) were then applied to simulate developmental mamelons within the tooth. Between the mamelons, Shade Occlusal Clear (Renamel Hybrid) was added to aid in the final translucency. Shade B-Zero microfilled composite (Renamel [Cosmedent]) was then overlain to cover the hybrid composite. The microfilled composite exhibits a more translucent color than the hybrid resin for a more natural appearance. A final layer of Renamel Enamel Light microfill (Cosmedent) was placed as a value modifying layer. The composite was then polished with Sof-Lex discs (3M ESPE), going from coarse to extra-fine, utilizing all 4 polishing grits. A final polish with FlexiBuff wheels (Cosmedent) impregnated with Enamelize (Cosmedent) gave the restoration its final luster.
 |
|
| Figure 8. Diagnostic wax-up demonstrating the desired leveling of the incisal edges. | Figure 9. Postoperative full-face photo (1:10 magnification). |
 |
 |
| Figure 10. The putty matrix with the facial areas removed. | Figure 11. The putty matrix placed on the model for incisal plane position. |
 |
 |
| Figure 12. Postoperative smile showing corrected incisal plane and lower lip. | Figure 13. Postoperative retracted smile (1:2 magnification). |
 |
|
Figure 14. Postoperative retracted smile (1:1 magnification). |
The central incisors set up the entire treatment. When they were complete and level, direction was turned to the lateral incisors and then the cuspids. At each step, the putty matrix was used to ensure that the correct incisal plane would be established, and proper color progression in the composites was established in the process. Polytetrafluoroethylene (Teflon) tape (Plumber’s Tape [Home Depot]), was used between adjacent teeth to prevent the teeth from bonding together. When all of the proposed teeth were completed, the patient was dismissed and scheduled for a follow-up visit a week later. Photos were taken for evaluation prior to the next appointment. This follow-up visit corrected minor defects, and the teeth were repolished (Figures 12 to 14).
|
Practice Management Ramifications: Dentrix
|
|
Amy Morgan |
DISCUSSION AND CLOSING COMMENTS
Coordination of the multitude of appointments and in-house lab base procedures must be very precise so that no steps are missed. In addition, efficient, clinically-based, dental software applications are also extremely valuable to deliver excellent patient treatment. To help us in these matters, our office has been a Dentrix (Henry Schein) user for more than 12 years. The addition of computers in the operatories several years ago has allowed us to be fully computerized with no paper patient charts for more than 6 years. The entire treatment plan is placed in the patient’s virtual chart, with each step spelled out in detail. Clinical notes are stored electronically for access anywhere. Proper documentation of composite shades allows us to easily retrieve this and other treatment-related information in the future. BOTOX injection site dosages and locations are documented on paper and then scanned into the document center. The office runs very well, and the patients can tell from the moment they walk into the practice that everything concerning their treatment always progresses very smoothly. It gives our office a distinction over others that not only are we technologically advanced, but our treatment is also going to be what is best for the patient.
A comfortable dental environment is better for the patients, staff, and doctor. At the end of the day, everyone goes home knowing that the very best dentistry is done using minimally invasive techniques when appropriate.
References
- Chiche GJ, Pinault A. Esthetics of Anterior Fixed Prosthodontics. Chicago, IL: Quintessence Publishing; 1994.
- Morley J. The role of cosmetic dentistry in restoring a youthful appearance. J Am Dent Assoc. 1999;130:1166-1172.
- Morley J, Eubank J. Macroesthetic elements of smile design. J Am Dent Assoc. 2001;132:39-45.
- Blitz N, Steel C, Willhite C. Diagnosis and Treatment Evaluation in Cosmetic Dentistry: A Guide to Accreditation Criteria. Madison, WI: American Academy of Cosmetic Dentistry; 2000.
- Kokich VO, Kokich VG, Kiyak HA. Perceptions of dental professionals and laypersons to altered dental esthetics: asymmetric and symmetric situations. Am J Orthod Dentofacial Orthop. 2006;130:141-151.
- Dawson PE. Functional Occlusion: From TMJ to Smile Design. St. Louis, MO: Mosby; 2007.
- Kois J. Functional Occlusion 1 [course manual]. Seattle, WA: Kois Seminars; 2008.
- Carruthers J, Carruthers A. BOTOX use in the mid and lower face and neck. Semin Cutan Med Surg. 2001;20:85-92.
Dr. Peck is a third generation dentist practicing in Cincinnati. He graduated from the Ohio State University College of Dentistry in 1985, and completed his residency at the University of Pittsburgh Medical Center. He has been focusing his practice over the past several years on full-mouth reconstruction and cosmetic treatments with a high-tech approach. Dr. Peck is an accredited member of the American Academy of Cosmetic Dentistry and a Fellow of the International College of Dentists. He is a member of the ADA, active in the Cincinnati Dental Society, and is treasurer and chairman of Utilization Review/Quality Assurance. He also is on the Board of Directors of Dental Care Plus, a Cincinnati-based dental insurance company. Dr. Peck can be reached via e-mail at fred@pecksmiles.com.
Disclosure: Dr. Peck is an unpaid consultant to Henry Schein Practice Solutions, on an as-needed basis.
Dr. Shuman is president of Pride Institute and is well known in the dental community for his leadership and expertise in the areas of strategic relations, emerging technologies, Internet strategy, practice management, and marketing. The Pride Institute’s goal is to utilize its reputation of integrity and fairness as a foundation in educating the community within the field of emerging technologies. He previously served as vice president of clinical education and then vice president of strategic relations for Align Technology for 7 years. He is a member of Dentistry Today’s Dental Advisory Board and has been listed in Dentistry Today’s Leaders in Continuing Education from 2004 to 2008, and is currently listed as a Leader in Dental Consulting. He is proud to be collaborating in this exciting new Dentistry Today article series. He can be reached via e-mail at lshumani@msn.com. Follow Dr. Lou Shuman on Google+, on Twitter (@LouShuman) or subscribe to Lou Shuman’s posts on Facebook.
Disclosure: Dr. Shuman reports no conflicts of interest.
Ms. Morgan serves as the CEO of Pride Institute. She is a dental consultant and international lecturer. Over the years, Ms. Morgan has facilitated the successful revitalization of thousands of dental practices using Pride Management Systems. She can be reached at amym@prideinstitute.com.
Disclosure: Ms. Morgan reports no conflicts of interest.

