

A previous dentist had performed a pulpotomy on tooth No. 18 to get the patient out of pain, but the patient still had percussion and biting sensitivity. The canals were very calcified and curved. I performed endodontic treatment and checked my file, and it came up short—literally!
The severity of the canal created a file separation with a size 30/.04. The odds of rotary file separation are 7 times greater than for hand files. The probability of separating a file in an apical third is 6 times greater than in the coronal and middle thirds of the canals.
Cyclic fatigue and torsional stress are the 2 main causes of breakage for NiTi endodontic files. Sometimes it can be a manufacturer defect or operator error as well.
 |
 |
| Figure 2. The x-ray of the completed case reveals 4 canals, each with independent apicies and the separated file in the mesiolingual canal. | Figure 3. This image shows a different angle of the post-op. Should we be worried about the file that separated? |
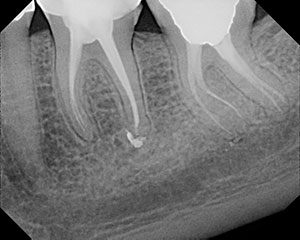 |
| Figure 4. The one-year recall showed the file still in place with no periapical pathology or symptoms after core buildup. |
Cyclic fatigue is when a material has repeated stress placed on it during a period of time. Ultimately, this repetition breaks the material. It’s similar to taking a piece of wire and bending it back and forth until it separates.
Torsional stress is when an object is twisted with an applied force. When a portion of material is locked into place and the rest continues to rotate, a breaking point is reached, and breaking or snapping occurs.
I told the patient about the file separation and documented it in the chart, which is the standard of care. I did not want to try to remove the file to make the x-ray look good. This would have removed more precious dentin and made the x-ray look worse.
This was a vital case with no lesion. I was already at the apex with a size 15 hand file and a previous size 25/.04, so I knew based on the studies that the outcome was going to be favorable.1 A lesion would have reduced the chance for success by only 5% to 7%.2,3
For the record, any file can separate. Don’t buy into those marketing schemes!
At the one-year recall, the area looked good, and the patient was asymptomatic.
References
- Crump MC, Natkin E. Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. J Am Dent Assoc. 1970 Jun;80(6):1341-1347.
- Fox J, Moodnik RM, Greenfield E, Atkinson JS. Filing root canals with files radiographic evaluation of 304 cases. N Y State Dent J. 1972 Mar;38(3)154-157.
- Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005 Dec;31(12):845-850.
Dr. Short attended the Medical College of Georgia (MCG) School of Dentistry to attain a DMD degree in 1999. In 2002, he earned his postdoctorate degree in endodontics from Nova Southeastern University and then became a Diplomate of the American Board of Endodontics in 2009. Dr. Short is an expert consultant in endodontics to the Georgia Board of Dentistry and assistant clinical professor at the Dental College of Georgia in Augusta. He also has published articles in several magazines and peer-reviewed journals including Dentistry Today, Inside Dentistry, Rolling Out Magazine, Upscale Magazine, and the Journal of Endodontics. He has lectured throughout the United States and the Caribbean. Dr. Short is endorsed by the American Association of Endodontists speakers bureau, and his private practice, Apex Endodontics PC, is located in Smryna, Ga. Dr. Short also has authored a book, Getting to the Root of Your Problem: 365 Days of Inspirational Thinking. He can be reached at dr.short@yahoo.com.
Additional Short Case Studies
Pulp Must Be Vital With an Open Apex


