
The success rate for non-surgical root canal treatments has been shown to be very high.1-3 Nonetheless, wet-fingered dentists are always eager to improve their root canal treatments diagnostically and technically. This includes scenarios in which dentists want to better visualize the treatment sites radiographically and intraorally or have the ability to locate calcified canals better. Furthermore, while we obviously want to improve the quality of our root canal treatments, we also strive to perform them faster. This may be especially crucial when dealing with endodontic emergencies or anxious patients.
This article will present a discussion, with demonstrations via clinical cases, on how to improve root canal treatments while also being able to diagnose and treat cases more efficiently. All this is thanks to new age tools and techniques that are now available to every dentist.
Enhanced Diagnosis
A common and fundamental issue in endodontics is with the challenges found in making a proper diagnosis. Ask yourself the following question: Do you really know what the problem is when a tooth with previous root canal treatment is symptomatic but nothing significant appears in a periapical radiograph? This is often the case when assessing maxillary molars that are superimposed radiographically with the zygoma and sinus. Does one really know the precise nature of a tooth with root resorption by means of traditional imaging and clinical examinations? Can dentists precisely diagnose a hairline vertical fracture under an old restoration or the presence of a pulp stone? These are just some of the limitations that dentists have faced for decades. However, the following advances in 3-D cone beam computed tomography (CBCT) imaging and enhanced magnification can make these issues things of the past.
 |
 |
| Figure 1. Tooth No. 14, with buccal swelling. | Figure 2. Tooth No. 14 appears (nearly) normal in 2-D periapical radiographs. |
 |
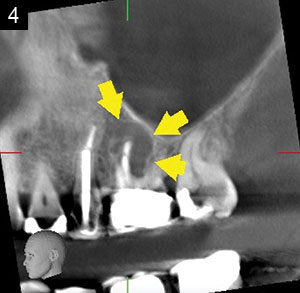 |
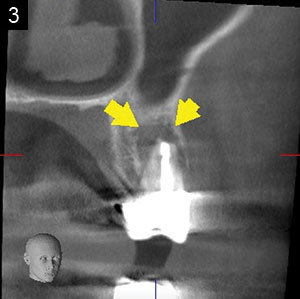
| Figures 3 and 4. CBCT imaging, showing a significant MB lesion/pathology in tooth No. 14. |
 |
| Figure 5. Clinical view of tooth No. 10, with hard and soft tissues appearing normal. |
Three-Dimensional Radiographic Imaging
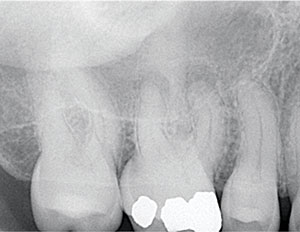
With good CBCT imaging, dentists can now diagnose many cases better and faster than ever before. The moment the digital scan appears on the computer and is interpreted, an experienced clinician may diagnose the issue at hand. For instance, a symptomatic tooth may appear normal in traditional 2-D imaging, but a quality 3-D scan quickly and precisely shows the apical pathology4-6 (Figures 1 to 4).
Clinical problem: Traditional 2-D imaging doesn’t reveal any (or enough) information, especially when the tooth is superimposed with the maxillary sinus and zygoma.
Solution: Take a CBCT scan of the same site instead of having to perform a surgical or nonsurgical endodontic access of the tooth.
In the resorption case involving Figures 5 to 7, it is difficult, perhaps impossible, to determine the exact location of the defect vertically and horizontally by means of 2-D imaging and clinical evaluation. However, with a 3-D scan, one can quickly, precisely, and atraumatically (without raising a surgical flap) determine the true extent of the problem.
Clinical problem: Root resorption is noted in a periapical radiograph, but its true extent is unknown.
Solution: Take a CBCT scan of the site instead of performing a more painful, expensive, and traumatic surgical flap evaluation. It should be stressed that not all endodontic cases require CBCT imaging. Yet, as demonstrated, when clinical and 2-D radiographic imaging do not provide enough information, 3-D radiographic imaging has proven itself to provide faster and, more importantly, better information than any other diagnostic protocol previously available. It has also been shown that the incorporation of 3-D imaging very often alters treatment plans when compared to 2-D imaging.5 Figures 8 and 9 illustrate 2 of the newest CBCT units.
 |
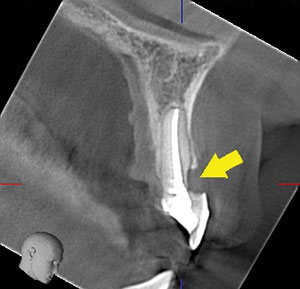 |
| Figure 6. A periapical radiogragh, showing tooth No. 10 with cervical resorption. | Figure 7. A sagittal CBCT image, clearly showing the extent and location of resorption. |
 |
 |
| Figure 8. Orthophos SL 3D CBCT unit (Dentsply Sirona). | Figure 9. Veraview X800 CBCT unit (J. Morita USA). |
Endodontic Access Preparations
Preparing endodontic access is one of the most difficult, time-consuming, and potentially risky procedures. This is especially so when dealing with calcified or heavily restored teeth.3 To help clinicians avoid mishaps and locate calcified canals more precisely and efficiently, Dentsply Sirona has developed the first, and only one of its kind, nonsurgical endodontic access guide (Figures 10 to 13). The SICAT Endo/ACCESSGUIDE (Dentsply Sirona) is similar to 3-D guided surgical implant stents, but it is made precisely and specifically for endodontics. It is produced by means of seamlessly incorporating the information from their 2-D Schick 33 sensors (Dentsply Sirona) and 3-D imaging (Orthophos SL 3D [Dentsply Sirona]) cone beam units and software (SICAT Endo and Sidexis 4 [Dentsply Sirona]). In turn, dentists now have the ability to do much better, safer, and faster endodontic access preparations, especi
ally in complex cases.7,8
Clinical problem: Calcified teeth that are difficult to locate and access and that increases the risk of perforation during access preparation.
Solution: Use a CBCT-guided ACCESSGUIDE (endodontic stent).
 |
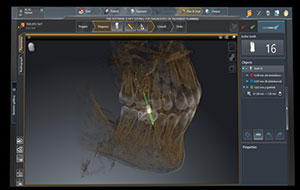 |
| Figure 10. Note (near) root access perforations in teeth Nos. 24 and 25. | Figure 11. SICAT Endo CBCT guided access planning software (Dentsply Sirona). |
 |
| Figure 12. CBCT guided endodontic SICAT Endo/ACCESSGUIDE (Dentsply Sirona). |
Enhanced Magnification
Once a tooth is accessed, it is important to evaluate it internally for canals, perforations, vertical fractures, and pulp stones. This can best and most quickly be done with the use of enhanced magnification and illumination. That includes quality, high-powered dental loupes with an overhead LED light or, even better, with a dental microscope (Figures 14 to 16).
A case in point is the ability to more easily and frequently locate MB2 canals of maxillary molars. This is a canal that dentists notoriously have issues in treating, as it’s often located under a dentin shelf and is very calcified.9,10
It is also important to mention the significance of locating internal fractures that could not be diagnosed without enhanced magnification and illumination. If left undiagnosed, a tooth with a hairline fracture would be bound to fail following endodontic treatment due to its underlying mechanical, not endodontic, problem. By diagnosing such a fracture early in the treatment process, the patient clearly receives better treatment and avoids unnecessary root canal therapy (Figures 17 to 19).
 |
 |
| Figure 13. The ACCESSGUIDE, in position for the endodontic access drill. | Figure 14. Extaro 300 dental microscope (Carl Zeiss). |
 |
 |
| Figure 15. A-Series microscope (Global Surgical). | Figure 16. Designs for Vision loupes with DayLight LED illumination. |
Additionally, enhanced magnification means a better and faster ability to locate canals, hairline fractures, and pulp stones, among other things. The following 2 clinical problem and solution scenarios highlight this:
Clinical problem: Tooth No. 3, with a small restoration and no apparent pathology, requires endodontic treatment, but with no clear etiology.
Solution: During endodontic treatment, evaluate the tooth internally under very high magnification.
Clinical problem: Endo is needed in a tooth with a calcified pulp chamber (Figure 20).
Solution: Use enhanced magnification with illumination (ie, a microscope or powerful dental loupes with LED light) for evaluation and treatment inside the endodontic access (Figures 21 to 24).
 |
 |
| Figure 17. Preoperative radiograph of symptomatic tooth No. 3. | Figure 18. Initial access view of tooth No. 3 with very low magnification. |
 |
| Figure 19. View of a vertical hairline fracture (red arrow) in tooth No. 3 that was only seen under high magnification with a dental microscope (Extaro 300). |
Instrumentation
Another part of the endodontic treatment protocol that has seen very practical and exciting advances is that of canal instrumentation. Thanks to advances in file designs and metallurgy, we can now use instruments better and faster than ever before.
A common issue with instrumentation, especially in very calcified and curved canals, is that of root canal transportation. This is especially an issue when using larger stainless steel hand files. With the advent of Glidepath NiTi files, it’s been shown that canal curvatures can be followed better than with hand files. In turn, this reduces canal transportations.11,12 Glidepath NiTi files may be considered as the mechanized, narrow taper, and very flexible version of traditional small-hand stainless steel files. These NiTi Glidepath files are commonly offered in tapers of .01 to .04. Quite simply, with these files, dentists can better negotiate calcified and curved canals (Figures 25 and 26).
Another advancement is found in the availability of reciprocating NiTi instrumentation.13 This was introduced by Dentsply Sirona Endodontics with its WaveOne system. The current generation is the WaveOne Gold system (Dentsply Sirona Endodontics), with 4 available file sizes and controlled memory (it can be pre-curved to enable easier endodontic access in patients with limited openings) (Figure 27). The Brasseler USA version of NiTi reciprocating files is the EndoSequence Reciprocating (ESR) system (Figure 28). The benefits of such instrumentation have caused these file systems to become very popular. The learning curve of using such systems has been improved, and their ability to resist file fractures and follow root curvatures has been shown to be better than many rotary NiTi files.14,15 In addition, the ability to perform all or most of the instrumentation with one file means improved efficiency and less room for error as fewer steps and instruments are needed than with traditional NiTi file systems.
 |
 |
| Figure 20. Tooth No. 3, with a calcified pulp chamber and apical lesions. | Figure 21. View of accessed tooth No. 3 with very low magnification. |
 |
 |
| Figure 22. View via a microscope of a pulp stone inside accessed tooth No. 3. | Figure 23. View of the pulp floor groove from MB1 to MB2 under pulp stone. |
 |
 |
| Figure 24. Final tooth No. 3 root canal treatment of 4 canals. | Figure 25. Scout .02 and .04 NiTi files (Brasseler USA). |
 |
 |
| Figure 26. WaveOne Gold Glider .02 NiTi file with controlled memory (Dentsply Sirona Endodontics). | Figure 27. WaveOne Gold NiTi reciprocating files (Dentsply Sirona Endodontics). |
 |
| Figure 28. ESR NiTi reciprocating files (Brasseler USA). |
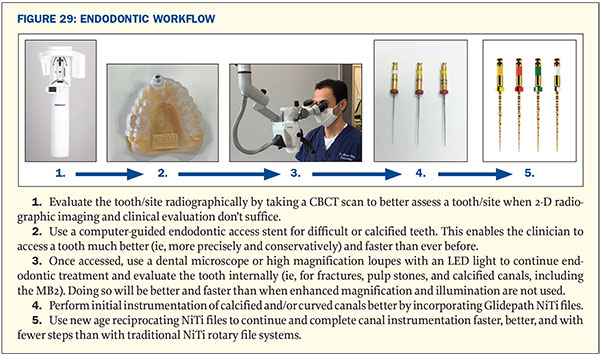
A Modern Endodontic Workflow Protocol
Figure 29 presents a step-by-step clinical workflow using new age tools and techniques. This is a modern endodontic protocol that will enable the clinician to improve and speed up root canal treatments, from diagnosis to instrumentation.
 |
CLOSING COMMENTS
It’s impressive to see how clinical endodontics has improved in recent years. Thanks to advances in 3-D imaging, enhanced magnification, and NiTi files engineered to better manage calcified and curved canals, we can more predictably perform quality root canals. Thanks to these instruments, we can now perform nonsurgical root canals better and faster, unlike ever before!
References
- Burry JC, Stover S, Eichmiller F, et al. Outcomes of primary endodontic therapy provided by endodontic specialists compared with other providers. J Endod. 2016;42:702-705.
- Fernández R, Cardona JA, Cadavid D, et al. Survival of endodontically treated roots/teeth based on periapical health and retention: a 10-year retrospective cohort study. J Endod. 2017;43:2001-2008.
- Peters OA, Peters CI, Basrani B. Cleaning and shaping the root canal system. In: Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis, MO: Elsevier; 2016:474-531.
- Scarfe WC, Levin MD, Gane D, et al. Use of cone beam computed tomography in endodontics. Int J Dent. 2009;2009:634567.
- Ee J, Fayad MI, Johnson BR. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J Endod. 2014;40:910-916.
- Low KM, Dula K, Bürgin W, et al. Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod. 2008;34:557-562.
- Buchgreitz J, Buchgreitz M, Mortensen D, et al. Guided access cavity preparation using cone-beam computed tomography and optical surface scans—an ex vivo study. Int Endod J. 2016;49:790-795.
- Krastl G, Zehnder MS, Connert T, et al. Guided endodontics: a novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent Traumatol. 2016;32:240-246.
- Buhrley LJ, Barrows MJ, BeGole EA, et al. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod. 2002;28:324-327.
- Görduysus MO, Görduysus M, Friedman S. Operating microscope improves negotiation of second mesiobuccal canals in maxillary molars. J Endod. 2001;27:683-686.
- Patiño PV, Biedma BM, Liébana CR, et al. The influence of a manual glide path on the separation rate of NiTi rotary instruments. J Endod. 2005;31:114-116.
- van der Vyver P. Creating a glide path for rotary NiTi instruments: part one. International Dentistry SA. 2011;13:6-10.
- Ahn SY, Kim HC, Kim E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: a systematic review of in vitro studies. J Endod. 2016;42:1009-1017.
- Yang Y, Shen Y, Ma J, et al. A micro-computed tomographic assessment of the influence of operator’s experience on the quality of WaveOne instrumentation. J Endod. 2016;42:1258-1262.
- Goldberg M, Dahan S, Machtou P. Centering ability and influence of experience when using WaveOne single-file technique in simulated canals. Int J Dent. 2012;2012:206321.
Dr. Haas is a certified specialist in endodontics and lectures internationally. He is a Fellow of the Royal College of Dentists of Canada and is on staff at the University of Toronto Faculty of Dentistry and the Hospital for Sick Children. He maintains a full-time private practice limited to endodontics and microsurgery in Toronto. He can be reached at haasendoeducation.com.
Disclosure: Dr. Haas reports no disclosures.
Related Articles
“Root Cause” on Netflix: Can Root Canals Make You Sick?
Clinical Tips for Instrumenting Calcified Canals
The Infamous MB2 Canal: How to Find It and Treat It

