
In part 1 of this 4-part series of articles, clinical pearls related to diagnostic procedures were discussed. In part 2, implant insertion will be addressed.
CREATING AND CORRECTING AN OSTEOTOMY FOR IMPLANT PLACEMENT
The ideal position for an implant is the center of the prosthetic tooth to be constructed. The abutment should be able to be positioned 1.5 to 2 mm lingual to the labial surface of the future restoration to permit room for metal, opaque, and porcelain.1 To avoid damaging adjacent teeth with the twist drill, placement of nonparallel implants may be necessary. In this regard, abutment angulations can be corrected with angled or custom abutments.2 Ultimately, implants should be placed in a manner that is restoratively reasonable and anatomically feasible.
The initial position for an osteotomy is marked with a small round bur (No. 2), or it may be beneficial to mark the spot with a larger round bur (No. 4) to prevent chatter of the twist drill. To reduce chatter, an alternate method to using the implant handpiece employs a No. 6 or No. 8 round diamond in a high-speed handpiece with copious irrigation and gentle pressure. Position of the osteotomy can be checked by placing a probe across the buccal of the adjacent teeth. Ideally, the center of the osteotomy should usually be located 4 mm from the probe (2 mm for implant radius and 2 mm for buccal bone).
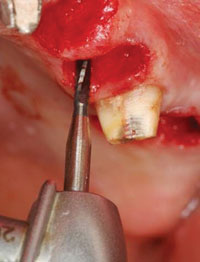 |
| Figure 1. Lindemann side-cutting (Brasseler USA) for lateral movement of osteotomy. |
There are several techniques to establish a stable position to place the twist drill when developing an osteotomy on a narrow or irregular ridge: use a thin, pointy 1.7-mm pilot drill (Salvin Dental Specialties) or high-speed handpiece with a small round bur to mark the alveolar crest. If there is adequate bone height and the ridge widens apically, flatten the alveolar crest with a diamond. When dealing with a thin ridge and it is desired not to lose any vertical bone height (eg, maxillary anterior area), another method to create a steady starting point consists of taking a round bur from the palatal side of the alveolar crest and creating a groove one to 2 mm deep and extend it halfway through the ridge.
In general, when initiating an osteotomy, drill to 5 mm and place a direction indicator to check its angulation. If the orientation is not correct, it is easy to fix when the osteotomy is 5 mm deep. If the osteotomy needs to be repositioned in a horizontal direction, use a Lindemann side-cutting bur (Brasseler USA) to move the osteotomy laterally (Figure 1). It is more efficient than trying to drag a twist drill laterally, which is not designed for side cutting.
 |
| Figure 2. Periosteal elevator placed parallel to submandibular undercut. It is not placed deeply. The osteotomy is created parallel to the periosteal elevator. |
To avoid perforating the lingual cortex of bone in the posterior mandible, where there may be an undercut (eg, submandibular fossa), place the periosteal elevator parallel to the bone, under the lingual flap. The elevator should not be pushed far apically; it is being used to provide guidance with regard to the degree of undercut present in the submandibular space. Drill the osteotomy parallel to the periosteal elevator, if this angle is restoratively reasonable (Figure 2). Position discrepancies with regard to implant inclination can be corrected with angled or custom abutments. Alternatively, to avoid angling the implant too much, the ridge can be augmented on the buccal to facilitate more advantageous placement.
During osteotomy preparation, after penetrating through the cortical bone, if something hard is hit—stop. One of several possible anatomical objects has been encountered, depending on the osteotomy location: adjacent tooth, buccal or lingual cortical plate, subantrum cortical bone, roof of the inferior alveolar canal, or inferior border of the mandible. It will be necessary to stop or redirect the twist drill, and it may be prudent to get a radiograph to determine what was encountered.
To reduce a patient’s postoperative discomfort, the following suggestions are made: use sharp burs, maintain continuous irrigation, avoid pressure on the handpiece, keep the periosteal elevator on the bone, and avoid pressing on the soft tissue during retraction. If any brown color is seen when drilling bone, it is being overheated. To avoid “burning” the bone, 50 mL/minute of irrigation is needed.3 The amount of generated heat is related to the drill diameter, thus with larger burs, make sure intermittent pressure is used. Do a “bone dance”—one second on, 2 seconds off (up and down). Burning bone may result in postoperative pain and possible nonintegration of an implant.
 |
|
Figure 3. A finger can be used to direct the head of the handpiece to ensure proper angulation of the osteotomy. |
With regard to the handpiece, it should not be leaking water when it is not in use. If it is, remove the water line from the motor, stretch it out, realign the tubing, and check to see if there is an air bubble. When a handpiece becomes locked in place, do not wiggle it, rotate it, or go in reverse; otherwise it will be damaged. Stop, disengage the twist drill, and rotate it out with a forceps. When developing an osteotomy, it may be beneficial to direct the head of the handpiece apically or laterally with the index finger of the hand not holding the handpiece (Figure 3). This technique provides excellent angulation control. If the head of the handpiece is pointing out of the mouth while preparing an osteotomy, stop, reassess the situation, and reorient it, because the angulation of the osteotomy as it relates to the opposing dentition is incorrect. When preparing an osteotomy for mandibular implants, the top of the handpiece is aimed at the inner aspect of the palatal cusp of the maxillary teeth, and while developing an osteotomy for maxillary implants, the handpiece is directed at the inner aspect of the buccal cusp of the mandibular teeth. This orientation is used to ensure that the central fossa of the crown to be restored on the implant is placed so that cusps of the opposing arch go into the central fossa.
Implant insertion is usually a routine procedure. However, if one wall is missing at the crest, sometimes the implant does not engage the osteotomy well and spins at the orifice. If this situation arises, or when inserting an implant into an osteotomy with a partially missing wall at the crest (eg, dehiscence), tip the implant to the side and engage a wall of the osteotomy at an angle. Once the tip of the implant is engaged, by both the buccal and lingual walls, then straighten it up to correct the angle and drive the implant into the osteotomy. Then place a bone graft and a barrier to regenerate the deficient wall. When the buccal wall is missing, anot
her technique that may help seat the implant and prevent it from being displaced to the buccal includes tapping the lateral and lingual walls.
MANAGEMENT OF BLEEDING PROBLEMS
Bleeding during implant placement can originate from soft tissue or bone. To control hemorrhage from soft tissue, inject anesthetic with 1/50,000 epinephrine and apply direct pressure. If bleeding is from an arteriole and a fine spray is being emitted from the tissue, apply pressure and it will usually rapidly subside. Continued bleeding may require a blood vessel to be clamped with a mosquito hemostat and then tied with a resorbable suture. If the blood vessel is not visible, try deep suturing to ligate the vessel. To halt bone hemorrhaging, various techniques can be used: inject anesthetic with epinephrine directly into a nutrient canal and/or twist gauze and hold it in place with a periosteal elevator; or burnish the bone to try to occlude it; or place a bone graft material into a defect which may obtund bleeding. Bleeding from an osteotomy can be managed by placing a direction indicator into the site or by inserting an implant into the completed osteotomy.
If bleeding develops from inadvertent penetration into in the floor of the mouth, an anesthetic with epinephrine can be used to induce vasoconstriction followed by applying firm pressure with gauze. When performing gauze tamponade, place one thumb inside and index finger outside the mouth and apply prolonged pressure. If a hematoma develops, do not cut it, because that may promote further hemorrhage. Ligation of the bleeding blood vessel is the preferred treatment. Prior to flap closure, the hemorrhaging must be controlled, because continued bleeding under the flap may cause the tongue to be displaced and the patient could develop a breathing problem.4
ACHIEVING PRIMARY STABILITY WHEN THERE IS A SPINNER
If there is poor primary stability after implant placement, there are several options to correct this problem. One option is to create a deeper osteotomy if apical bone is available. Another choice would be to employ a wider implant when bone and space exist. Still another technique that can be useful consists of adding bone with an amalgam carrier, condensing the bone, and then placing the implant.5 An osteotome or a drill (not moving) one size smaller than the implant to be placed can be used to condense bone laterally and create an orienting space for implant insertion.
SOFT-TISSUE MANAGEMENT
1. Flap Design and Handling. Factors to be considered in flap design include the following: access for instrumentation, maintenance of blood supply, preservation of tissue topography, allowance for identification of vital structures, and providing for closure. There are numerous variations in flap designs that will be dictated by the number of implants to be placed and the surrounding anatomical structures. Currently, crestal incisions are usually employed. Envelope flaps are routinely used with and without papillary sparing incision to provide access for limited areas to receive implants (Figure 4). Incisions should score the bone, thereby incising the periosteum when elevating a full thickness flap.
 |
|
Figure 4. Papilla sparing incision leaves 1.0 mm of the papilla adjacent to the tooth. |
For the fully edentulous mandible, crestal posterior and midline vertical releasing incisions are sometimes employed to provide access. In the edentulous maxilla, similar incisions can be made. Some clinicians move the crestal incision labially around the incisive papilla to avoid transecting the contents of the nasopalatine canal. Alternately, vertical releasing incisions can be made distal to the canal region and posteriorly as needed. However, it should be noted that an incision through the canal region does not usually have a detrimental affect.
Flaps should be hydrated periodically so they do not become desiccated. After a long procedure, hydrate the flap and stretch it out. When one tooth is being treated, extend the flap as much as necessary to provide adequate access for surgery. Frequently, when employing an envelope flap, there is a need to include an additional papilla beyond the tooth adjacent to the site being treated to achieve tension-free access and avoid tearing the flap. If treating a deep periodontal defect (eg, 8 mm) on a single tooth, an envelope flap across 3 teeth will rarely provide adequate access. Extend the envelope flap one tooth distal or mesial to the defect being treated and create a vertical releasing incision. There are no elastic fibers in gingiva, so the incision line will heal without scarring.
2. Using Periosteal Elevators and Suctioning. Place an elevator to the desired depth and make sure it is underneath the periosteum on bone. There are several techniques that can be employed when using a periosteal elevator: rotate clockwise, then counterclockwise; vertical elevation, wiggle out and in; move along the incision line.6 Other ideas with respect to using a periosteal elevator are listed. When elevating thin tissue, use the thumb to oppose the reflection—this helps avoid tissue tears. It is useful to sharpen periosteal elevators. Have the assistant retract the flap with the periosteal elevator during surgical procedures to avoid operator fatigue. It is beneficial when working with one assistant to create sufficient reflection to permit him or her to retract the flap with the high-speed suction tip. This frees up the assistant’s other hand to handle instruments, etc.
 |
|
Figure 5. Tying flaps back can improve visibility during surgical procedures. |
After flaps are elevated, the elevator should always remain on the bone, because if it compresses, the tissue there will experience increased postoperative swelling. In addition, have the assistant suction the bone; if the tissue is suctioned, there will be increased edema. Suctioning should be done in a sweeping motion, because when the suction tip pokes at the tissue, it can pick up the mucosa and not function efficiently.
3. Tying Flaps Back To Increase Visibility. In the beginning of a procedure, restraining flaps to enhance visibility takes an extra few minutes, but it can be worthwhile with regard to saving time and facilitating access (Figure 5). If both sides of the arch are simultaneously being treated, tie the lingual flaps to each other. When only one side is surgerized, secure the lingual flap to the teeth on the other side of the same arch. Sometimes it also is beneficial to fix the buccal flap to the cheek. Another technique is to tie the flap to itself. For example, on the lingual, loop through the mesial of the flap (buccal to lingual) and tie it to the distal of the flap (lingual to buccal) and pull it tight. The tension created by the sutures keeps the tissue reflected.
4. Suturing and Surgical Knots. As a general rule, suture movable tissue to fixed tissue rather than fixed tissue to loose tissue. Snug sutures down, but do not tie them tight, because tension can result in pressure necrosis, and the sutures may tear through the tissues.7 When suturing, the needle should
engage 2 to 3 mm of tissue, and sutures should be placed every 3 to 5 mm along the incision line. Leave ears of 2 to 3 mm long after cutting the suture or it may unravel. A surgeon’s knot is usually all that is necessary to close an incision line (2 ties clockwise and one tie counterclockwise). When synthetic or naturally resorbing sutures are used, the clinician can add another clockwise knot to prevent unraveling. Note that additional ties do not add to the strength of a correctly tied knot—they only add to its bulk. Tie all the knots on the same side of the incision line. When tightening a knot, pull in a direction parallel to the incision line, not perpendicular to it. Final tension of final throw should be as nearly horizontal as possible. A sling suture (lasso) around the implant will pull the flap tightly around the implant. When selecting a suture material, keep in mind how long tensile strength lasts for different types of suture materials: plain gut (7 to 10 days), chromic gut (10 to 14 days), and Vicryl (40% at 21 days).
 |
|
Figure 6. Diagram showing how to close a T-vertical releasing incision. |
When closing a vertical releasing incision and the fixed tissue is thin, before trying to suture, slightly raise the fixed tissue with an elevator so that the suture needle can fit through the tissue without tearing it. To close a vertical releasing incision distal to the osteotomy site (T-shaped incision), use a figure-8 or criss-cross suture as follows (Figure 6). At the distal of the crestal (horizontal) incision, engage the buccal aspect of the horizontal flap, then cross the vertical incision line and enter the fixed tissue on the distolingual and knot it. Do not cut the suture yet. Now engage the buccal aspect of the fixed tissue distal to the vertical releasing incision and suture this to the distolingual aspect of the movable flap across the vertical incision and tie a knot. The figure-8 suture will pull the T releasing incision together. If desired, a figure-8 suture can also be used over an extraction site to draw the margins of the gingiva towards each other.
Over a barrier membrane, there is an increased tendency to observe tissue dehiscences. To help avoid this, place horizontal mattress sutures using an absorbable suture (eg, Vicryl). Then reinforce these sutures with interrupted sutures. Conceptually, the mattress suture provides additional strength to resist muscle pull (eg, buccinator or mentalis muscle). However, suture technique is not a substitute for appropriate flap release and passivity of closure. After an incision is sutured, use wet gauze to compress the flap, and then take a probe to check to see that the flap is well coapted (gently brush the probe across the suture line to find sections of tissue not engaged well).
 |
5. Critical Factors Affecting Papilla Height in the Aesthetic Zone. After a surgical procedure, if the distance between the osseous crest to the contact point between teeth is < 5 mm, the papilla will usually return (98% of the time).8 When the distance is 6 or 7 mm, the chance of the papilla filling the embrasure is, respectively, 56% and 27%. According to Garber et al,9 in the aesthetic zone, the height of the average papilla that forms adjacent to an implant is dependent on the type of restoration adjacent to the implant (Table). The determining factor for papilla height adjacent to a single implant is based on the interproximal bone height of the adjacent tooth.10 This is true even if there is severe bone loss on the tooth to be extracted. Accordingly, before implant placement, the sulcus of the adjacent tooth needs to be probed to predict future papillary height. The supracrestal fibers of the adjacent tooth maintain the papillary height. On the day of insertion of a single implant crown in an edentulous space, the papilla will not completely fill the embrasure 90% of the time, because after an extraction, the papilla recedes.11 However, within one year, 80% of the interdental spaces will be filled.11
 |
 |
|
Figures 7a and 7b. Shrinkage of papilla after an extraction (a) and reformation after restoration (b). The col disappears and reappears. |
 |
|
Figure 8. Short papilla between implants at sites Nos. 5 and 6. Average height of the papilla between implants is 3.4 mm. |
After an extraction, it doesn’t matter if an edentulous area is temporarily restored with or without a flipper; the col area shrinks and becomes keratinized. Subsequently, after an implant and a temporary crown are placed, the papilla and its col reform (Figures 7a and 7b). On the other hand, if an implant is placed into an extraction site and is immediately provisionalized, it helps maintain the papillary form and height. It also has been noted that if a healing abutment is not removed after initially being placed, there will be less recession, because the junctional epithelium was not disturbed.12 With respect to the final aesthetic outcome, it does not matter if a flipper or a temporary crown are immediately used, since the attachment level on the adjacent natural teeth determine the final papillary height.13
Between dental implants the average height of the papilla is 3.4 mm (Figure 8).14 According to Tarnow, et al,14 the papilla between implants will attain the following heights (crest of bone to contact point): 2, 3, 4, and 5 mm, respectively, 16.9%, 34.7%, 37.9%, and 5.6% of the time. Ninety percent of the papilla will be between 2 to 4 mm in height. The reduction of papillary height compared to natural teeth is due to the absence of supracrestal gingival fibers.
 |
 |
 |
|
Figures 9a to |
Based on the above information, the following conclusions can be drawn to with respect to maximizing anterior aesthetics. If there is a choice with respect to which sites can be used for implants to replace missing maxillary anterior teeth (eg, Nos. 7 to 10), it will be more aesthetic if 2 implants are not placed next to each other, since a short papilla will develop. It would be preferable to place implants at sites Nos. 7 and 10, or Nos. 7 and 9, or Nos. 8 and 10 (Figures 9a to 9c). If only 2 adjacent teeth are missing, consider placing one implant and a cantilever. In addition, for an optimum aesthetic result, it is preferable to use an ovate pontic.15,16 Sometimes it will be necessary to place a connective tissue graft to augment the soft tissue under the ovate pontic. If Nos. 8 and 9 are the 2 adjacent teeth that are missing, 2 implants can be placed, and an aesthetic result can be attained by lengthening the contact area in the midline. The real difficulty arises when Nos. 7 and 8 or Nos. 9 and 10 are the adjacent missing teeth, because this will result in asymmetry with respect to the papillary heights on the contralateral side.
IMMEDIATE IMPLANT PLACEMENT
A major potential problem after immediate implant placement is recession of the buccal gingiva. Therefore, several clinical factors need to be considered prior to placing an immediate implant in the premaxilla. It is advisable to only do immediate implants when there is a low smile-line, there is no recession on the tooth, the buccal plate is present, and the gingiva is healthy. It is also prudent to only attempt them when there is a thick biotype (85% of patients present with a thick flat gingiva)17 and an adequate amount of gingiva. The biotype is considered thick if you place a probe within the sulcus and you cannot see the probe; it is labeled as thin if the probe can be seen.18 On average, thin biotypes have 0.7 mm more recession than thick biotypes.18 Upon extraction, the buccal plate needs to be assessed with a probe, and immediate placement should only be done when there is an intact buccal plate of bone (the thicker the better). To help avoid recession, the implant’s trajectory should be directed to the cingulum of the future crown to preserve additional buccal bone. If there is a thin biotype, place the implant a little more palatally to decrease the chance of recession and to prevent a titanium shadow from appearing through the thin gingiva. In addition, place it a little more apically to attain a good emergence profile and avoid development of a ridge lap. Pertinently, it needs to be remembered that subsequent to insertion of standard or wide body implants in solid bone, recession was noted at the time of prosthesis placement (0.4 versus 1.15 mm) and increased at one year postinsertion (0.8 versus 1.45 mm).19 With regard to sites undergoing immediate placement, recession has also been noted.20,21 In case of recession, it is sometimes necessary to restore the adjacent teeth so that gingival disharmony can be corrected.
 |
| Figure 10. Lindemann bur used in anterior socket to create on ledge on the palatal wall. |
After an extraction in the premaxilla, the osteotomy for an immediate implant is usually initiated in the palatal bone of the socket one half to two thirds of the distance to the apex. The site can be marked several different ways: with a round bur directly into the bone (horizontally) and then after a purchase is attained, the twist drill is directed more vertically; the round bur can be used laterally to sink into the bone to create a ledge; a Lindemann bur can be employed to make a ridge on the palatal wall (Figure 10) or a pilot drill with a sharp point can be used to demarcate a purchase point for the twist drill.
When preparing an osteotomy for an immediate implant that is not going to be submerged, it is advisable to widen the orifice on the palatal wall of the osteotomy to accommodate the flare of the implant and healing abutment, or use a straight healing abutment. Otherwise, the flare of the coronal portion of the implant or component will force the implant labially and possibly into an undesirable position. If the implant achieves stability with 30 to 40 Ncm torquing force, then placement of an immediate provisional resin crown is an appropriate protocol.22 The provisional temporary should be kept out of occlusion.
WOUND HEALING RATES
Repair time for specific tissues significant to the implant surgeon are listed: epithelium—after a 12-hour lag time, 0.5 mm to 1 mm daily;23 connective tissue—0.5 mm daily;24 bone—50 µm daily (1.5 mm per month);25 sinus lift—1 to 2 mm bone per month; Schneiderian membrane—heals at the rate of epithelium. Furthermore, epithelium cannot cover a wound until connective tissue is present, because epithelium is avascular and needs a connective tissue base. With respect to healing after flap surgery, there is a specific sequence of biologic events. Initially, after suturing, the mucoperiosteal flap is attached to bone (or soft-tissue flap) by a blood clot (zero to 24 hours). At one week, the clot has been replaced by granulation tissue. If the flap is adjacent to a tooth, it is connected via an epithelial attachment and young fibroblasts. In any of the healing scenarios, after 2 weeks, fibroblasts produce collagen and the flap is attached to bone via immature collagen fibers. Hiatt, et al26 used a tensiometer on sacrificed dogs and reported that the force needed to separate a flap from bone was as follows: at 2 to 3 days (225 gm), one week (340 gm), and at 2 weeks, 1700 gm of force could not displace the flap. In general, flaps are attached in 10 days (dog model) and will not be easily displaced.27 Bear in mind that smaller mammals heal at a slightly faster rate than humans. With regard to post-surgical timing for restorative therapy, Dowling, et al28 suggested that after flap surgery, clinicians should wait about 8 weeks to allow for collagen maturation before proceeding with final restorations. However, if there was a thin periodontium, recession may manifest itself up until 6 months; therefore, in areas of aesthetic concern, delay of the prosthesis for 5 to 6 months may be needed to ensure gingival margin stability. Subsequent to placement of temporary restorations, 2 to 3 months should be allowed for sculpting of tissues; sometimes it can take longer.29 After a particulate graft is placed, 4 to 6 months is needed for graft calcification before an implant should be inserted30 and after a cortical block graft, 4 to 5 months is required for healing.31 Four to 6 months after placing a particulate graft, before scheduling implant surgery, it is advantageous to anesthetize the area and sound the bone with a 30-gauge needle to determine if the graft is calcified.
In a future issue of Dentistry Today, “Clinical Pearls for Surgical Implant Dentistry, Part 3: Adjuctive Implant Procedures” will be presented.
References
- Harrison L, Huffman T, Goldfogel M. All-porcelain labial margin for ceramometal crowns. J Esthet Dent. 1992;4:154-158.
- Sethi A, Kaus T, Sochor P, et al. Evolution of the concept of angulated
abutments in implant dentistry: 14-year clinical data. Implant Dent. 2002;11:41-51. - Eriksson AR, Albrektsson T. Temperature threshold levels for heat-induced bone tissue injury: a vital-microscopic study in the rabbit. J Prosthet Dent. 1983;50:101-107.
- Niamtu J III. Near-fatal airway obstruction after routine implant placement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:597-600.
- Hahn J. Clinical uses of osteotomes. J Oral Implantol. 1999;25:23-29.
- Weiss CM, Weiss A. Principles and Practice of Implant Dentistry. St. Louis, MO: Mosby; 2001:134-136.
- Silverstein LH. Principles of Dental Suturing: The Complete Guide to Surgical Closure. Mahwah, NJ: Montage Media; 1999:70-75.
- Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992;63:995-996.
- Garber DA, Salama MA, Salama H. Immediate total tooth replacement. Compend Contin Educ Dent. 2001;22:210-218.
- Choquet V, Hermans M, Adriaenssens P, et al. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001;72:1364-1371.
- Jemt T. Regeneration of gingival papillae after single-implant treatment. Int J Periodontics Restorative Dent. 1997;17:326-333.
- Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited. J Clin Periodontol. 1996;23:971-973.
- Jemt T. Restoring the gingival contour by means of provisional resin crowns after single-implant treatment. Int J Periodontics Restorative Dent. 1999;19:20-29.
- Tarnow D, Elian N, Fletcher P, et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003;74:1785-1788.
- Garber DA, Rosenberg ES. The edentulous ridge in fixed prosthodontics. Compend Contin Educ Dent. 1981;2:212-223.
- Miller MB. Ovate pontics: the natural tooth replacement. Pract Periodontics Aesthet Dent. 1996;8:140.
- Olsson M, Lindhe J. Periodontal characteristics in individuals with varying form of the upper central incisors. J Clin Periodontol. 1991;18:78-82.
- Kan JY, Rungcharassaeng K, Umezu K, et al. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. J Periodontol. 2003;74:557-562.
- Small PN, Tarnow DP. Gingival recession around implants: a 1-year longitudinal prospective study. Int J Oral Maxillofac Implants. 2000;15:527-532.
- Lindeboom JA, Tjiook Y, Kroon FH. Immediate placement of implants in periapical infected sites: a prospective randomized study in 50 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:705-710.
- Lin CD, Chang SS, Liou CS, et al. Management of interdental papillae loss with forced eruption, immediate implantation, and root-form pontic. J Periodontol. 2006;77:135-141.
- Saadoun AP. Immediate implant placement and temporization in extraction and healing sites. Compend Contin Educ Dent. 2002;23:309-318.
- Engler WO, Ramfjord SP, Hiniker JJ. Healing following simple gingivectomy. A tritiated thymidine radioautographic study. I. Epithelialization. J Periodontol. 1966;37:298-308.
- Ramfjord SP, Engler WO, Hiniker JJ. A radioautographic study of healing following simple gingivectomy. II. The connective tissue. J Periodontol. 1966;37:179-189.
- Misch CE. Bone augmentation for implant placement: keys to bone grafting. In: Contemporary Implant Dentistry. 2nd ed. St Louis, MO: Mosby; 1999:453.
- Hiatt WH, Stallard RE, Butler ED, et al. Repair following mucoperiosteal flap surgery with full gingival retention. J Periodontol. 1968;39:11-16.
- Werfully S, Areibi G, Toner M, et al. Tensile strength, histological and immunohistochemical observations of periodontal wound healing in the dog. J Periodontal Res. 2002;37:366-374.
- Dowling EA, Maze GI, Kaldahl WB. Postsurgical timing of restorative therapy: a review. J Prosthodont. 1994;3:172-177.
- Chee WW, Donovan T. Use of provisional restorations to enhance soft-tissue contours for implant restorations. Compend Contin Educ Dent. 1998;19:481-486.
- Tischler M, Misch CE. Extraction site bone grafting in general dentistry. Review of applications and principles. Dent Today. 2004;23:108-113.
- Pikos MA. Block autografts for localized ridge augmentation: Part II. The posterior mandible. Implant Dent. 2000;9:67-75.
Dr. Greenstein is a graduate of New York University College of Dentistry (NYUCD) and received his MS from the University of Rochester. A Board Diplomate and Fellow of the American Academy of Periodontolgy (AAP), he is a former clinical professor in the Department of Periodontology and Implant Dentistry at NYUCD. He currently maintains a private practice in Freehold, NJ. Dr. Greenstein has authored more than 100 articles on periodontal and implant therapy and has been the recipient of the Gies Award for contributions to literature from AAP and the Hirschfeld Award from the Northeast Society of Periodontology. He can be reached at (732) 780-1450 or via e-mail at ggperio@aol.com.
Disclosure: Dr. Greenstein reports no conflicts of interest.
Dr. Cavallaro is a member of the Academy of Osseointegration and a Fellow of the Greater New York Academy of Prosthodontics. He maintains a private practice of prosthodontics and surgical implant dentistry in Brooklyn, NY. Dr. Cavallaro is a former associate clinical professor in the Department of Periodontology and Implant Dentistry at the New York University College of Dentistry. He has published multiple articles on surgical and prosthetic implant dentistry and has lectured on these subjects for the past 20 years. He can be reached at docsamurai@si.rr.com.
Disclosure: Dr. Cavallaro reports no conflicts of interest.
Dr. Tarnow has a certificate in periodontics and prosthodontics, is a Diplomate of the American Board of Periodontology, and has a private practice in New York City. Dr. Tarnow is a former professor and chairman of the Department of Periodontology and Implant Dentistry at the New York University (NYU) College of Dentistry. He is also a recipient of the Master Clinician Award from the American Academy of Periodontology and Teacher of the Year Award from NYU. He has published more than 100 articles on perioprosthodontics and implant dentistry, and has co-authored 3 textbooks, including one in 2008 entitled Aesthetic Restorative Dentistry. He has lectured extensively internationally. He can be reached at dennis.tarnow@gmail.edu.
Disclosure: Dr. Tarnow reports no conflicts of interest.

