
Editor’s Note: Dr. Bailey wrote a related CE article in the November 2000 issue of Dentistry Today. Becuase of the timely nature of this topic, this article updates and expands the previous article with the most current information.
The American Academy of Sleep Medicine (AASM) reports that 100 million Americans of all ages fail to get a good night’s sleep, and the average American gets 243 hours less sleep per year than in 1969.1 Management of sleep disorders is an expanding area in medical care, and practicing physicians are now paying more attention to sleep as a primary or secondary risk factor for many common conditions. In addition, dentists now participate in the recognition and treatment of sleep disorders, and this article is intended to review basic concepts of sleep disorders and the role of the dentist in the care of affected patients.
DENTISTRY’S EXPANDING ROLE
Every dentist who evaluates and treats patients with existing hypertension, bruxism, fatigue during the day, headaches, or jaw pain of muscular origin is seeing a patient who may have a sleep problem that contributes to the primary diagnosis.
Dentistry’s role and involvement in the treatment and management of a sleep-disordered patient may be indirect or direct.
THE INDIRECT APPROACH
This method pertains mainly to the recognition of what is suspected to be a sleep disorder problem, educating the patient, and appropriately referring the patient for care. This referral may be to the patient’s primary care physician or to a physician that specializes in sleep medicine. Examples of sleep disorders that might be recognized by the dentist are2:
•Insomnia–the inability to fall asleep or to maintain sleep.
•Restless limb syndrome–a condition where the arms and/or legs jerk or move involuntarily during sleep, often disrupting the affected individual’s sleep or that of the bed partner.
•Jet lag–a problem that may lead to fatigue in someone who crosses multiple time zones on a regular basis and experiences an irregular sleep/wake schedule.
•Narcolepsy–a condition where the person experiences sudden bouts of sleepiness for no apparent reason during the day.
THE DIRECT APPROACH
In this situation the dentist works directly with the patient in the management of their sleep disorder. The sleep disorders that the dentist will most often treat are referred to as sleep-related breathing disorders (SRBDs). Included here are2:
•Snoring–loud sounds made during sleep with inhalation, caused by the vibration of unsupported tissues in the airway.
•Obstructive sleep apnea (OSA)–the cessation of breathing during sleep that lasts for 10 seconds or longer. It is often associated with an arousal from sleep and may result in a measurable fall in oxygen saturation.
•Upper airway resistance syndrome (UARS)–a condition associated with increased blockage of the airway or increased airway resistance, usually without a fall in oxygen saturation.
•Hypopnea–a narrowing of the airway, which leads to a decrease in airflow and a reduction in respiratory effort. This could be considered as a partial airway obstruction, with an associated fall in oxygen saturation.
•Obstructive sleep apnea hypopnea syndrome (OSAHS)–a frequently used term that combines the findings of obstructive sleep apnea and hypopnea into a single category.
SRBDs account for the vast majority of sleep disorders, and are very prevalent in our society. As noted, these disorders can be associated with a reduction in the patient’s blood oxygen saturation during sleep, and snoring is also a common finding. Patients with SRBDs also experience sleep fragmentation, or frequently disrupted or broken sleep. This pattern is associated with frequent waking, and the affected person often rises in the morning feeling tired, as though they had not slept during the night.3
SLEEP BRUXISM
Another condition associated with SRBD is sleep bruxism.4 Traditionally, bruxism has been viewed as a condition that occurs in relation to stress or some other behavioral issue, or in association with occlusal problems. A recent study demonstrated that bruxism is controlled through the central nervous system and is linked to the dopaminergic system.5 It is well recognized that bruxism mainly occurs during NREM (nonrapid eye movement) stage 2 sleep and to a lesser degree during REM (rapid eye movement), which are not the deepest stages of sleep. REM sleep is characterized by the rapid movement of the eyes during sleep with specific EEG activity, whereas in NREM sleep there is the absence of eye movement with a specific and different level of EEG activity.
The AASM views sleep bruxism as a parasomnia, a disorder that intrudes into sleep and occurs during sleep but is not a principal sleep disorder. The AASM further defines sleep bruxism as “a stereotyped movement disorder characterized by grinding or clenching of the teeth during sleep.”2
| Table 1. Odds of Sleep Bruxism (Compared to Population Without the Condition)4 | ||
|
Ohayon et al4 found that sleep bruxism may occur in association with snoring and sleep apnea. In fact, the odds ratio of sleep bruxism occurring with SRBD is higher than bruxism occurring with anxiety or stress (Table 1). (Note: The study assessed the entire spectrum of bruxers and found that those at risk for the additional conditions, ie, increased risk factors, were associated with sleep bruxism.) In this same study it was reported that one third of the patients with sleep bruxism reported feeling tired in the morning.
As these conditions are routinely seen in dental offices, dentists are well positioned to be of assistance to the SRBD patient by fabrication of an intraoral appliance that repositions the mandible to assist in opening the airway. Here the dentist will treat the patient with an appliance after consulting with the patient’s physician or the sleep specialist. In many instances the patient may undergo an overnight sleep study, called a polysomnogram, to determine if they have sleep apnea or OSAHS, and how severe is the condition.
Many patients who are diagnosed with sleep apnea or OSAHS are introduced to nasal continuous positive airway pressure (CPAP) as a means of treatment. CPAP consists of a mask that fits tightly over the nose, and a small generator attached via a hose to the mask forces air through the no
se to pneumatically open the airway. This method of treatment is very effective but is often poorly tolerated because of restrictions to movement during sleep, air leaks around the mask, and drying of the nose and/or throat. Another problem with CPAP is that this treatment may not be effective in the apnea patient who is not sleepy.6
In addition, patients who snore but do not have apnea (who comprise a large number of those with SRBD) and do not find CPAP helpful may require an alternate type of therapy. Historically, surgery has often been the most commonly sought procedure because patients likely are more aware of it as a treatment for snoring. Surgery, particularly soft tissue revision surgery, may have limited success and is irreversible. Today, an oral appliance that repositions the jaw is a well-accepted option that offers a high degree of success.7 However, many patients are not aware that it even exists as a treatment option for SRBD.
| Table 2. Therapeutic Measures for the Patient With Sleep Bruxism and Snoring: The Role of the Oral Appliance | ||
1. Patient currently using nasal CPAP 2. Continue to use CPAP; consider an oral appliance as substitutive therapy such as for traveling or when the CPAP machine cannot be used. Re-evaluate every 6 to 12 months for effectiveness. 3. Oral appliance therapy with mandibular repositioning device 4. Surgical consultation |
Table 2 provides a guide for determining the role of oral appliance therapy in the management of patients with sleep bruxism and snoring.8
THE EFFECTS OF SRBD
SRBD has been shown to be associated with a wide variety of sequelae. Some of the effects of SRBD include9:
(1) increased incidence of motor vehicle accidents (it has been estimated that $12.4 billion in accident-related costs is related to sleep deprivation)10
(2) excessive daytime sleepiness
(3) memory loss, especially short term
(4) impotence or loss of sex drive
(5) hypertension and other related cardiovascular diseases
(6) morning headaches
(7) a feeling of general fatigue.
The overall goal of treatment of SRBD is to improve the quality of the individual’s sleep and hence improve their quality of life. The objectives in the treatment and management of SRBD include:
(1) improving sleep quality
(2) reducing daytime fatigue
(3) improving sleep for the bed partner
(4) reducing or eliminating headaches
(5) controling or better managing hypertension and related health conditions
(6) improving memory
(7) improving libido
(8) reducing the risk of motor vehicle accidents
(9) improving quality of life.
Certain findings observed by the dentist should raise suspicion that the patient suffers from SRBD. Some of the following are considered to be prevalent in these patients9:
(1) Increased neck size. If the neck size is 17” or more in a male and 15.5” in a female be sure to inquire about snoring and apnea.
(2) Advancing age. With age there is an increased risk for SRBD. Consider that by the age of 40 the prevalence of snoring is 40% in males and 20% in females, and by age 60 the prevalence is 60% in males and 40% in females.
(3) Increased weight. With increased weight the potential to snore or have OSAHS increases.
(4) Other family members snore or have apnea. There appears to be some genetic predisposition, but this is not well defined.
(5) Hypothyroidism. This condition is strongly correlated to SRBD.
(6) Smoking and alcohol use. There appears to be a greater incidence of SRBD in those who smoke or use alcohol on a regular basis.
(7) Hypertension. There have been numerous studies that correlate hypertension to sleep-disordered breathing. This appears to be related to an increase in sympathetic nervous system tone.11,12
(8) Enlarged tonsils and/or adenoids. The presence of these structures is often associated with SRBD, especially in younger patients.13,14
(9) Gastroesophageal reflux. The presence of this condition often accompanies SRBD because of negative esophageal pressures that are associated with negative pressures in the airway.
ORAL APPLIANCE THERAPY
 |
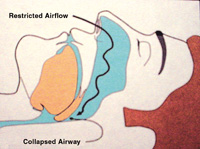 |
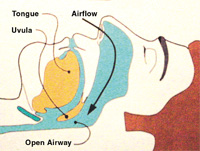
| Figure 1. Normal airway during sleep. | Figure 2. A snorer’s collapsed airway. |
 |
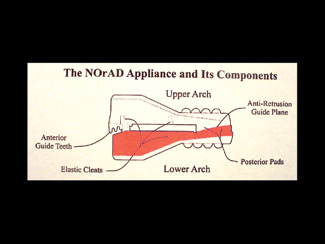 |
| Figure 3. Oral appliance opens the airway. | Figure 4. The Norad oral appliance. |
The use of oral appliances that reposition the mandible during sleep are becoming more widely accepted by the medical profession and by physicians who specialize in sleep medicine.15 The goal of an appliance is to maintain
an open airway during sleep as is illustrated in Figure 1. During sleep the airway in a snorer or sleep apnea patient collapses, causing a restriction in the airway that then may lead to snoring and to apnea if significant enough (Figure 2). Typically, oral appliances that are used to manage SRBD are comprised of maxillary and mandibular components that attach firmly to the upper and lower teeth in each arch, and are secured together in some manner that allows for repositioning of the mandible and movement of the tongue away from the back of the oropharynx and prevents the jaw and tongue from retruding into the airway, thus causing airway restriction or obstruction (Figure 3). In addition, the muscles that control the airway (and the mandible) are stretched in order to open or dilate the airway. There are many theories as to why this type of device works effectively. Schwab16 demonstrated that with mandibular repositioning the airway is opened, and the major impact is in the lateral dimension, not in the anterior-posterior dimension.
The advantages of using an oral appliance are that it is reversible, noninvasive, and generally convenient for the patient. It is less obtrusive than CPAP, and has a higher degree of success as compared with most surgical procedures.17 The availability of oral appliances has increased, and published studies have demonstrated their effectiveness for both snoring and sleep apnea. One study in particular that looked at a fairly large number of patients demonstrated the effectiveness of oral appliances for snoring and sleep apnea.7 Because dentists are acquainted with the use of intraoral appliances worn at night, the management of snoring with an oral appliance is best provided by the dentist. The ability to provide this service enhances the scope of the practice, and can have a positive impact on patients who suffer from SRBD.
In addition, most of the appliances available today also have the ability to manage sleep bruxism by virtue of posterior support, which allows them to function as do most bite splints that are used for TMJ conditions and managing bruxing during sleep. Based on the association of SRBD and sleep bruxism, those patients previously treated or considering conventional treatment with an occlusal splint or nightguard are logical candidates for an oral appliance that can also resolve snoring.
CASE REPORT
A 54-year-old patient presented based on the referral of a physician specializing in sleep disorders for consideration of an oral appliance to manage snoring. She had undergone several sleep studies in the past that were inconclusive for sleep apnea. Nasal CPAP had been considered, but she was unable to tolerate this treatment because of the fit of the mask, a complaint of facial and cervical pain, and dislodging of the mask during sleep.
She reported a positive history of loud snoring with frequent wakening during the night. She was always tired and was experiencing memory problems. She also reported depression. Her blood pressure was mildly elevated, but did not require medication. She was aware of grinding her teeth at night when she slept. In addition, she was a teacher who lived and worked overseas for most of the year. She visited the United States only once per year. As a result, treatment of most medical conditions, including her sleep disordered breathing, was not readily available.
It was determined that an oral appliance was indicated. Because of time limitations and for convenience the Norad appliance, which is an immediate use, semi-custom oral appliance for the management of snoring and sleep apnea, was selected. Other appliances in this category that the clinician may select to achieve similar objectives include the Therasnore (Distar) and the Silencer Custom (Integrated Health Technologies).
The Norad is first softened in boiling water, and is fit in the office. It offers 5 mm of vertical opening, and also allows for some anterior repositioning when the patient sleeps (Figure 4). In addition, the appliance provides posterior support for the management of bruxism.
The appliance was fabricated for the patient at the initial visit. This required 20 to 30 minutes; the appliance can be fit immediately without the need for laboratory processing. The appliance is available in one size and fits 90% of all patients who are candidates for an oral appliance. However, in using this device one should be cautious that all of the posterior teeth are in contact with the appliance. The dentist can expect this appliance to have a 2- to 3-year lifespan, depending on care and use. Had this patient not had the time restrictions because of her travel schedule, a custom fabricated, laboratory processed appliance could have been considered, although in many cases an appliance such as the one described is selected by the clinician.
Ten days after receiving the appliance the patient reported that her snoring was resolved, she was sleeping more peacefully, and her mood was improved. She also felt that she was not as tired during the day. At a follow-up visit a few days later she reported no discomfort with her occlusion, she had no discomfort in the face or jaws, and the temporomandibular joints were comfortable.
CONCLUSION
Sleep-disordered breathing (snoring and sleep apnea) is a condition that is becoming more common, and newer and more conservative approaches to treatment are constantly being sought. Dentists are now part of the team of health professionals that can assist these patients.
Acknowledgment
This article was written with the assistance of Michael Gelb, DDS, MS. The author wishes to acknowledge his participation in the development of this manuscript.
References
1. Regional Fulfillment Center: Getting the Sleep You Need Booklet. Washington, DC: Sleep Research Institute; 1998: No. SL-950.
2. The International Classification of Sleep Disorders: Diagnostic and Coding Manual. Westbrook, Ill: American Academy of Sleep Medicine; 1997:181-185.
3. Lee-Chiong T, Sateia M, Carskadon M. Sleep Medicine. Philadelphia, Pa: Hanley & Belfus; 2002.
4. Ohayon M, Li K, Guilleminault C. Risk factors for sleep bruxism in the general population. Chest. 2001;119:53-61.
5. Lobbezoo F, Naeije M. Bruxism is mainly regulated centrally, not peripherally. J Oral Rehabil. 2001;28:1085-1091.
6. Barbe F, Mayoralas LR, Duran J, et al. Treatment with continuous positive airway pressure is not effective in patients with sleep apnea but no daytime sleepiness: a randomized, controlled trial. Ann Intern Med. 2001;134:1015-1023.
7. Pancer J, Al-Faifi S, Al-Faifi M, et al. Evaluation of variable mandibular advancement appliance for treatment of snoring and sleep apnea. Chest. 1999;116:1511-1518.
8. Sher AE. Upper airway surgery for obstructive sleep apnea. Sleep Med Rev. 2002;6:195-212.
9. Kryger M, Roth R, Dement W. Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WB Saunders Co; 2000.
10. Dement W. The perils of drowsy driving. N Engl J Med. 1997;337:783-784.
11. Peppard, PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
12. Garcia-Rio F, Racionero A, Pino J, et al. Sleep apnea and hypertension: the role of peripheral chemorecptors and the sympathetic system. Chest. 2000; 117:1417-1425.
13. Postic W, Pasquariello P, Baranak C, et al. Relief of upper airway obstruction by adenotonsillectomy. Otolaryngol Head Neck Surg. 1986;94:476.
14. Marcus C, Loughlin G. Obstructive sleep apnea in children. Seminars Ped
iatric Neurology.1996;3:23-28.
15. Schmidt-Nowara W. Recent developments in oral appliance therapy of sleep disordered breathing. Sleep Breathing. 1999;3:103-106.
16. Schwab R. Imaging for the snoring and sleep apnea patient. In: Dental Clinics of North America. Attanasio R, Bailey D, eds. Phildelphia, Pa: WB Saunders; 2001:759-796.
17. Wilhelmsson B, Tegelberg A, Walker-Engstrom ML, et al. A prospective randomized study of a dental appliance compared with uvulopalatopharyngoplasty in the treatment of obstructive sleep. Apnea Acta Otolaryngol. 1999;119:503-509.
Dr. Bailey is a general dentist with offices in Englewood and Colorado Springs, Colo. His practice in these locations is restricted to the management of temporomandibular disorders, orofacial pain, related headaches, and the management of snoring and sleep apnea utilizing intraoral appliances. He has fellowships in the Academy of General Dentistry, the International College of Dentists, and the Academy of Dentistry International. He is a member of the Academy of General Dentistry, the American Academy of Sleep Medicine, the American Academy of Orofacial Pain, the American Headache Society, the American Pain Society, and the International Association for the Study of Pain.
Disclosure: Dr. Bailey has an ownership position in the company that manufactures the Norad appliance, which is marketed by Sullivan-Schein.


