




Dental caries remains one of the most common chronic diseases in humans. Approximately 80% to 90% of tooth decay in permanent teeth occurs in the pits and fissures located on the occlusal surfaces of posterior teeth. Diagnosing caries in these vulnerable sites often creates a diagnostic dilemma for dental professionals. Early pit and fissure decay often goes undetected by X-rays, visual inspection, and probing with an explorer, which can damage enamel surface integrity.
Ortek Therapeutics introduced the Ortek ECD, an electronic caries detection device that measures the conductivity of enamel. Powered by a 9-volt battery, this small, portable system has a base unit with a digital display, a handpiece with a dimensionally configured stainless steel tip that reaches into the bottom of a pit or fissure, and a reference lip hook. If the dentin-enamel junction is breached by demineralization, hydrostatic pressure within dentinal tubules allows minuscule amounts of conductive dentinal fluid to enter the breached enamel site, enabling the ECD to complete an electrical circuit.
Loss of minerals from enamel as a result of caries activity increases pore size and enamel porosity. As this demineralization progresses, more dentinal fluid enters the breached site. The increased fluid results in lower resistance, a higher current, and a rising digital caries score displayed from 0 to 100. A score of zero indicates no cavitated lesion, as intact tooth enamel is electrically non-conductive.
CASE REPORT
A 22-year-old patient came to the office complaining of tooth sensitivity when eating sweets. Clinical examination showed obvious decay in the disto-occlusal pit on the maxillary first molar (Figure 1, site 3). Upon further examination, the mesio-occlusal pit (Figure 1, site 2) was suspicious, but there was no evidence of cavitation from visual and radiographic methods, making a treatment decision difficult. A second mesio-occlusal pit appeared sound (Figure 1, site 1).
This case was ideal to evaluate the digital caries score indicated by the ECD, as there was an obvious cavitated lesion, a questionable site, and what appeared to be a sound site. After isolating the tooth with cotton rolls and thoroughly drying the occlusal surface with an air syringe, I gently placed the conductive tip into the bottom of the pits of each site. The ECD displayed the following readings. Site 1: 00, site 2: 04, and site 3: 93.
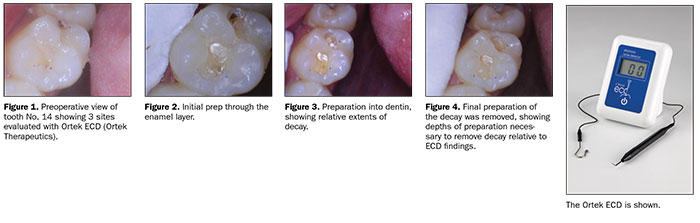 |
Following administration of local anesthesia, the tooth was prepared in each of the 3 sites. Once the enamel was removed, site 1 expectedly showed no decay, while sites 2 and 3 showed decay as discoloration and a soft feel with the explorer (Figure 2). Preparations were further advanced into the dentin (Figure 3). Once the decay was removed, we can see the relative depths of preparation necessary to remove all of the decay. Site 3 required deeper excavation relative to site 2, as indicated by the ECD (Figure 4). Following cavity preparation, the tooth was restored with a composite restoration, the occlusion was adjusted, and the restoration/tooth was polished.
The ECD scores proved extremely reliable relative to the depth of the caries lesions and the indication of a sound enamel site. In this case, the ECD was very effective in detecting a small cavitated lesion that may have normally gone untreated.
CONCLUSION
The ECD is highly efficacious, very affordable, and quick and easy to use. The ECD is a valuable new tool that can help diagnose and monitor early cavitated lesions in pit and fissures that often go undetected by x-rays, visuals, and tactile methods. Incorporating the ECD into my practice has numerous advantages, including dramatically enhanced patient care, a new profit center with a rapid return on investment, and building trust with current patients while attracting new ones.
For more information, call Ortek Therapeutics at (888) 323-0023 or visit ecddetect.com.
ABOUT THE AUTHOR
Dr. Zimbardi received his DDS degree from the New York University College of Dentistry in 1996. He received his bachelor’s degree in biology at the State University of New York at Binghamton. Dr. Zimbardi received his postdoctoral general Practice residency at Long Island Jewish Medical Center, New Hyde Park, NY from 1996 to 1998. His final year of residency was distinguished by being appointed chief resident.
He has been in private practice since 1998 and is currently a member of the following dental societies: Nassau County Dental Society, New York State Dental Association, the ADA, and Omicron Kappa Upsilon. Dr. Zimbardi is a member of the Peer Review Committee of the Nassau County Dental Society.








