
THE INDEX CASE
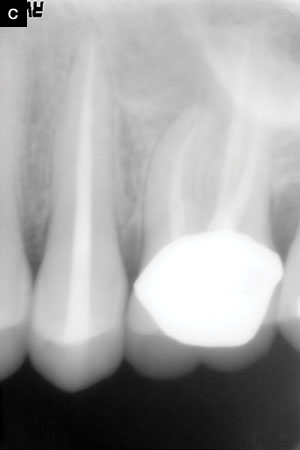
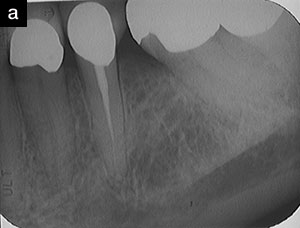
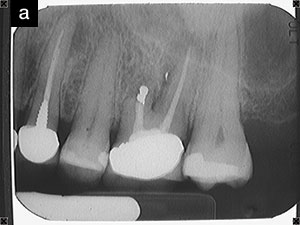
Medicine uses the term index case to denote the first documented patient with a particular problem or disease. Ashlee (Figure 1) presented in 2003 with a complaint of pain in her upper left quadrant as well as heat sensitivity. Despite the radiographic findings on the previously treated maxillary molar, clinical tests suggested that the pain was coming from the unrestored maxillary second bicuspid. Given her age at the time (late 30s), we did not suspect a cracked tooth, nor was there evidence of a crack when it was clinically examined under high magnification using the microscope. We were unable to elicit a history of trauma to the area as well. Unsure of the diagnosis and unable to identify an etiology for an endodontic problem on tooth No. 13, we scheduled her back for a re-evaluation 2 days later. The re-evaluation confirmed the initial findings of percussion sensitivity; no response to cold; and a delayed, building, lingering sensitivity to heat that can happen with end-stage pulpitis or early pulp necrosis. Other than the radiographic findings, the previously treated maxillary first molar and other teeth in the area tested as expected. With trepidation, we began treatment on the maxillary second bicuspid, accessing the pulp chamber using a surgical operating microscope (Global Surgical). We found a necrotic pulp chamber with no evidence of cracks or fractures. We placed Ca(OH)2, and her symptoms resolved immediately. We completed the RCT on the asymptomatic tooth 2 weeks later, and she elected to monitor the maxillary first molar.
Why Did the Pulp Die?
As dental students, we all became familiar with the commonly accepted belief that “occlusion doesn’t cause periodontal disease” and “occlusion doesn’t cause endodontic disease.” Both of these issues have had readily identifiable bacterial components. In one sense, with both diseases being narrowly defined as having a bacterial etiology, these beliefs may be true. In contrast, a TMD problem that is without a readily identifiable bacterial component will find many warring factions of gnathologists and TMD/TMJ experts, who often assign occlusal problems as the etiology of these TMD issues, seeking to address the problem with their particular interventions. Looking back on this index case, I can see those occlusal risk factors in this “workout queen” who was a personal trainer that operated her own gym. (Picture Arnold Schwarzenegger clenching his teeth at the bench press.)
 |
 |
 |
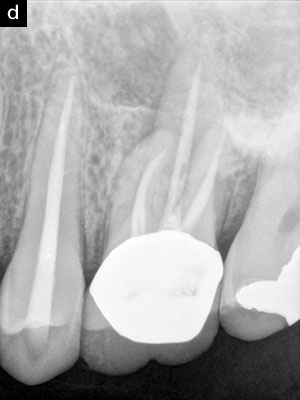 |
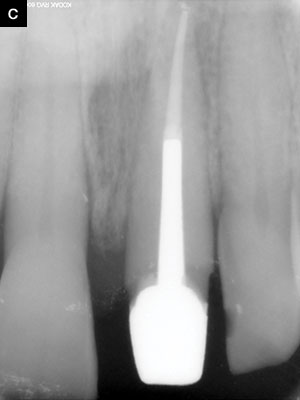
| Figure 1. (a) Preoperative projection radiography is unremarkable on the maxillary first bicuspid. (b) Access does not show any evidence of crack or fracture. (c) The postoperative radiograph, with symptoms having completely resolved. (d) Ten-year followup shows the tooth remains completely asymptomatic and within normal limits clinically. The maxillary first molar with radiographic findings also remained asymptomatic for this time period. |
The failure of the Endodontic Triad to predict success, and equally important to predict failure, has been noted in several articles in Dentistry Today.FN-1, 1-4 As W.D. Miller wrote in an 1890 article titled “Gangrenous Tooth-Pulps as Centers of Infection,” “The subject which I have in mind, not to discuss, but simply to propose to you for consideration or investigation, is one of very great interest to the dentist….”5 Herein, we wish only to propose to you for consideration or investigation in your practice that there may be a role of occlusion in the precipitation, or exacerbation, of both endodontic and periodontal problems. We propose that, lacking better language or categorization, that occlusal problems in patients presenting with complaints or clinical/radiographic findings manifest at the weakest link. When we say occlusal problems, we mean more than heavy function, but heavy parafunctional activity, such as diurnal/nocturnal clenching, grinding or both. The cause, or more likely, causes are not fully known, but are thought to be combinations of such things as airway disturbances, sleep disturbances, malocclusion, stress, substance use or abuse, and the restorations that clinicians are placing. We mean this in a way analogous to Casadevall’s Damage Response Framework that ultimately leads to tissue damage, a patient complaint, or both.
The Phoenix Abscess, Revisited
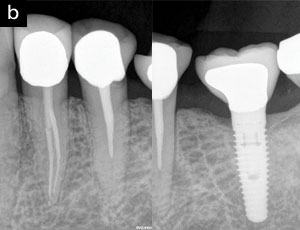
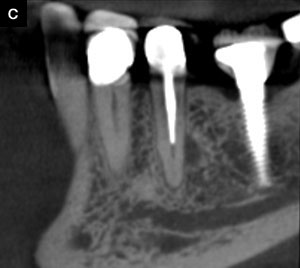
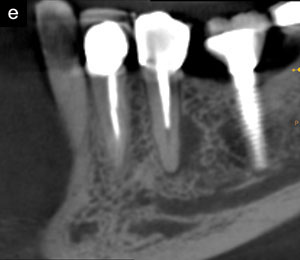
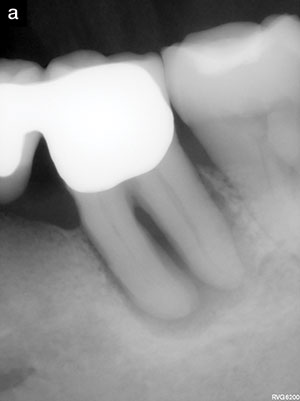
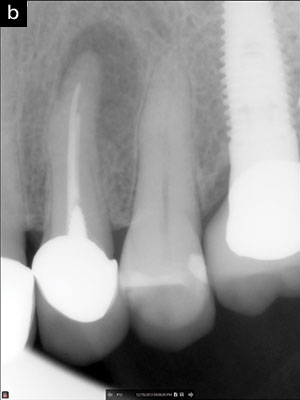
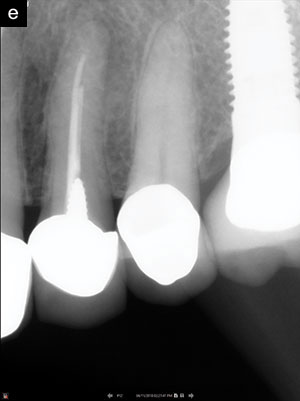
A phoenix abscess is defined as an acute exacerbation of a chronic periapical lesion; a lesion being the entity in the patient and not the radiographic finding, as is commonly, and incorrectly, described. We first saw Jennifer (Figure 2) in 2005 regarding symptoms involving her lower second molar (tooth No. 18). Her first molar had been removed. It was noted that there had been previous endodontic treatment on the lower second bicuspid, tooth No. 20. While the process-outcome on the bicuspid leaves much to be desired, the tooth was asymptomatic, and there were no clinical findings or radiographic evidence of apical periodontitis on the bicuspid, so we did not recommend any treatment on that tooth. A resorptive defect was discovered in her symptomatic molar, and she had the tooth removed and an implant-supported crown (ISC) placed in the No. 19 position. We saw her for other treatment over the years, including for her symptomatic lower first bicuspid in 2017. We ordered a preoperative CBCT scan to aid in treatment planning for the lower first bicuspid and discovered a small, lateral radiolucency in the CBCT scan that was then visible in hindsight on the projection radiograph. One wonders if it was there in 2005 but just not visible with film. We noted a suspicious area on tooth No. 20 on the PA projection radiograph and got a BW angle (Figure 2b, right) that looked within normal limits. Regardless, the crown on No. 20 was replaced with a porcelain-fused-to-zirconia (PFZ) crown and, within a year, the radiolucency increased, and she reported back with symptoms on that dead tooth—rising out of the ashes. One may note the wear facets on the PFZ crown that occurred within a year. We recently re-treated the tooth in 2 visits and placed a post (D.T. Light Post [BISCO Dental Products]) with a core (LuxaCore [DMG America]).
 |
 |
 |
 |
 |
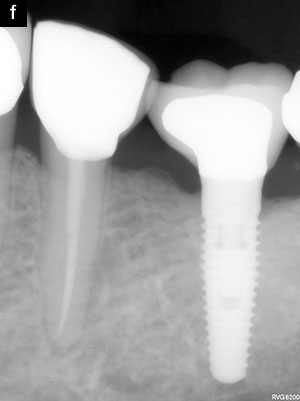 |
| Figure 2. (a) The scanned film on the lower second bicuspid from 2005 shows a thready fill but no radiographic evidence of apical periodontitis. (b1) At the time of treatment of the lower first bicuspid No. 21 twelve years later, there is perhaps a hint of a lateral radiolucency and a suspicion of decay at the distal of the lower second bicuspid No. 20. (b2) With that suspicion, a flat BW-angle to visualize the interproximal area between the implant and D No. 20 was taken at treatment time does not evidence decay at the crown margin. (c)The lateral radiolucency on No. 20 suspected in (b1) was confirmed with the pre-op CBCT scan at the same time No. 21 was treated. A new porcelain-fused-to-zirconia crown had been placed and, within a year, (d) developed wear facets and symptoms, and (e) an increased radiolucency was noted on the CBCT scan. (f) The post-op radiograph of the retreatment result. |
Restorative clinicians routinely place new indirect restorations on previously endodontically treated teeth without giving much thought to the existing endodontics. If a tooth has been asymptomatic, and there isn’t obvious evidence of coronal leakage or other radiographic findings, this is largely appropriate. This is in contrast with prevailing endodontic thought and recent recommendations from the American Association of Endodontics, which we believe not to be evidence-based, nor in the best interest of the patient. However, the reason the new indirect restoration is placed is important. Is it because the old indirect restoration has worn through or has fractured? Without excluding leakage and microbial contamination—something that is present in all cases, including symptomatic and asymptomatic—might these occasional flare-ups after placing new crowns on previously treated teeth be due to changes in the occlusion? It stands to reason that the crown broke for a reason. We don’t believe it was worn through the occlusal surface or lost all the occlusal porcelain because it was only hitting in function. Everything leaks, and there is bacteria everywhere, but there isn’t always a problem. Could it be a microbial problem manifesting in a different way? Buerger et al6 wrote:
Random, low-frequency exit from the nongrowing state may be a key element of a general microbial survival strategy, and the phylogenetic breadth of the organisms exhibiting such exit indicates that it represents a general phenomenon. The stochasticity of awakening can also provide a parsimonious explanation to several microbiological observations, including the apparent randomness of latent infections and the existence of viable-but-nonculturable cells (VBNC).
Thus, the bacteria remaining after prior endodontic treatment may be present in a dormant state, provoking little response from the host. A scout cell stochastically awakens, independent of environmental cues. Perhaps these changes in occlusion kick off some inflammatory changes in the host that facilitate reawakening or resuscitation of the already-existing bacteria from dormancy? Much remains to be learned, but what is clear from decades of endodontic research is that we do not eliminate bacteria from the root canal system, and, most of the time, our patients are fine.
 |
 |
 |
 |
 |
| Figure 3. (a) Initial radiographic presentation, consistent with a long-standing endodontic problem. (b) Interim treatment radiograph of the vital case with Vitapex. An effort was made to extrude material. (c) Short-term projection follow-up. (d) Pre-op CBCT scan, showing nearly complete loss of the buccal cortical plate and circumferential bone loss. (e) One-year follow-up CBCT scan in Vitapex, showing radiographic evidence of osseous regeneration and partial cortical plate reformation. We do not expect this case to fully resolve, nor do we have any illusions about curing the multiple problems with this tooth. We hope for a functional, asymptomatic retention of the tooth. Note the occlusal flattening of the occlusal surface of the lower second molar in (c) vs (a). She remains asymptomatic at one year. |
A Role in Periodontal Problems?
In our minds, there is some evidence for a possible role of occlusal problems in creating or exacerbating existing problems. The question then becomes “Can we reverse these problems with an occlusal intervention?” Amelia (Figure 3) presented in early 2018 with a complaint of pain for months in duration in her lower right quadrant, including sensitivity to cold and a bad taste in her mouth. She reported that the bridge from teeth Nos. 18 to 21 was placed in 2003. It appeared stable and serviceable upon examination. There were periodontal probings of 9-plus mm into the furcation, with exudate. However, and surprisingly, tooth No. 18 was not just responsive to cold, but very cold sensitive with lingering pain. This was inconsistent with the radiographic appearance of a necrotic tooth—that is, the radiographic presentation is consistent with a long-standing endodontic problem from a necrotic tooth. However, a necrotic tooth is inconsistent with her complaint of cold sensitivity and the clinical test results. With microscopic evaluation, we also noted crushed porcelain, marked faceting, and occlusal interferences. Therefore, we suspected an occlusal component to the periodontal problem. After repeated testing and careful clinical evaluation, we diagnosed her with a retrograde pulpitis in tooth No. 18 along with periodontal problems. It was recommended that she have the tooth removed and an implant-supported crown placed. The patient had been missing teeth Nos. 19 and 20 for a long time, and the CBCT scan revealed inadequate bone for an implant. The periodontist proposed tooth removal with ridge preservation for No. 18 and ridge augmentation for No. 20. She was dead-set against the bone grafting procedures on religiou
s grounds. In consultation with her restorative dentist and the periodontist, along with great trepidation and painting a picture of likely failure, we felt like we had little to lose in starting the endodontic treatment to see if we could resolve her symptoms. Along with the planned pulpectomy, localized scaling and an aggressive occlusal adjustment were done at the periodontist’s office. Access was made to a vital pulp as expected, very light instrumentation was done, and a calcium hydroxide and iodoform paste (Vitapex [Neo Dental International]) was placed. Her primary symptoms resolved quickly, and all of her symptoms resolved after occlusal adjustment.
 |
 |
 |
 |
 |
 |
 |
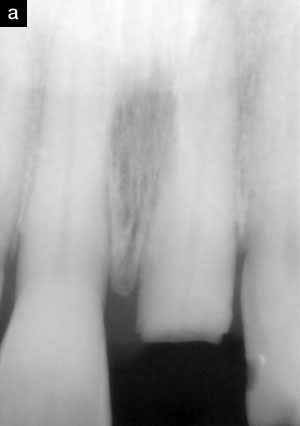
| Figure 4. (a) Pre-op projection radiograph of tooth No. 14 shows an asymptomatic radiolucency associated with tooth No. 12. (b and c) Eight years later, the patient re-presented under duress with an enlarged radiographic finding, including pain and swelling in the area of tooth No. 12. Aggressive occlusal relief of excursive interferences was done. (d) Swelling largely resolved over the next several weeks, with complete resolution in 6 weeks. (e) Projection radiography suggests a resolving PA finding at one year. (f) Two-year follow up. (g) Five-year follow up. The area remains asymptomatic and devoid of clinical findings. |
As a necrotic pulp was not the etiologic agent for the periradicular bone loss, nor the suppuration, we would not expect endodontic treatment to resolve those issues. Could the occlusal issues have played a role in the disease process? Did addressing these issues play a role in the healing and resolution of symptoms?
The Mother of All Occlusal Adjustments
Although many of the cases above could plausibly be assigned to a bacterial etiology, we believe that the occlusal issues played a role in the issues highlighted. Roger Lewis, MD, PhD, and an editor of the Journal of the American Medical Association (JAMA), remarks, “A single case can be very powerful, if it is so counter to prevailing thought that it forces the discipline to reconsider some of the foundational principles and beliefs.” In fact, a single case can prove something that a million cases cannot, just as a single black swan can prove that not all swans are white.
 |
 |
 |
 |
 |
| Figure 5. (a) The patient presents with the previous crown that has snapped off. (b to d) Elective endodontics, orthodontic extrusion and a cast post was fabricated. (e) At the 12-year follow up, we see the common patient complaint that the tooth with the crown “has gotten longer” but of course it’s the other teeth that have been worn, along with the lower incisors. Note that we readily see this pattern on anterior teeth with the crowned tooth being “longer,” but it is less easy to discern on posterior teeth, and often manifests with broken or sheared off cusps as seen in Figure 6. |
We first saw Analicia (Figure 4) in 2004 for a different issue, and she re-presented in 2005 regarding the maxillary first molar that had been treated, had periapical surgery, and then had a root amputation. We recommended the extraction of tooth No. 14. We also noted the radiographic finding on the asymptomatic maxillary first bicuspid; we had reason to believe that the endodontic treatment on that tooth was performed prior to 1995. We did not recommend any treatment on that tooth.
We continued to see Analicia for a variety of issues over the years, and it wasn’t until 2013 that she re-presented with pain and swelling on the maxillary first bicuspid. The radiographic finding had clearly enlarged. She was going through an extremely difficult time in her life personally and was under considerable duress and distress, along with having significant financial issues. We discussed options on this tooth and recommended either an ISC or periapical surgery, neither of which was financially viable for her, with extraction as a lower cost option. With little to lose, we suggested that the issue may have been brought about by stress-induced clenching/grinding, resulting in occlusal trauma from the tooth acting as an excursive guide. We dramatically cut away the buccal cusp and relieved the occlusion on the palatal inclines of the buccal cusp and the buccal inclines of the palatal cusp, leaving the tooth in centric contact only. Her restorative dentist had made her an acrylic NTI appliance (a tension-suppression system), which she had not been wearing. We advised her to begin wearing it as previously directed. We did not prescribe any antibiotics.
 |
 |
 |
| Figure 6. (a) The patient was referred to the prosthodontist from the restorative dentist after occlusal adjustments on the zirconia restoration on No. 14 failed to resolve symptoms. (b and c) Clinical examination reveals that the opposing porcelain of the PFM restoration on No. 19 has been extensively fractured away, along with fractured porcelain on many other restorations. Further examination notes include the loss of canine disclusion and that lateral movements have become group function. The patient reports that he has had off-and-on symptoms with No. 14 for some time and that it has recently been keeping him awake at night with discomfort. The pain could be replicated immediately upon a left working movement, and No. 14 appeared to still have excursive interferences after adjustment at the restorative dentist’s office. The patient was recommended to see the endodontist. |
We followed her very closely over the next weeks as her symptoms resolved and the swelling reduced. By 2 months, she was completely asymptomatic. She agreed to allow us to monitor her closely. She has remained asymptomatic in this area for more than 5 years now. Interestingly, about a year after this first incident, she went through another difficult time, had stopped wearing her NTI, and presented with similar symptoms and palpation sensitivity in the maxillary anterior segment. This time, we made her a QuickSplint (quicksplint.com) and then saw her at one week for a follow-up evaluation. At that appointment, she was doing much better, and her palpation sensitivity was gone. Here, assigning a strictly bacterial etiology to the problem stretches credulity to fantastic extremes.
What About Dental Implants?
Consensus of current practice is to place implants just out of light centric occlusion. Over time, teeth wear and the opposing tooth may erupt slightly, resulting in the implant being in a more pronounced centric contact. Considering the lack of a PDL, the implant effectively becomes the first stop. If the implant-supported crown is fabricated in gold, the restoration may wear similarly to the wear on the surrounding teeth. While porcelain doesn’t wear at the same rate as teeth, it does wear some and generally wears the opposing tooth at an increased rate (Figure 5). If the forces are too great, it will chip or fracture to re-establish occlusal harmony (or by breaking, de-establishing the lack of occlusal harmony). So, these 2 materials that have stood the test of time are not without their problems but are at least somewhat forgiving. By comparison, zirconia does not appreciably wear, nor is it likely to chip or fracture, so those forces will be absorbed by some other tissue, often the opposing tooth and/or bone or the bone surrounding the implant. Without going so far as predicting a cascade of implant failures over the next 10 to 20 years, we will not be surprised to see many implants failing, along with collateral damage to the bone or opposing teeth (Figure 6).
Durango is a very small community with one oral surgeon, one endodontist, one prosthodontist, and 2 periodontists. This affords us the opportunity, or responsibility/duty/obligation/burden, to see our own failures in a way that clinicians in a larger area might not see. We have had monthly breakfast study clubs for many years and have arrived at some conclusions not widely accepted in the dental community. When we see a necrotic No. 3 opposing a zirconia crown on a recently placed ISC, we know all the clinicians involved in treatment. We can discover why No. 30 was removed in the first place and what its treatment history was. As we have shown here, we have historical radiographs, often going back decades.
As a result of these observations, we have formulated the following hypothesis:
The Durango Hypothesis on Occlusal Trauma. Occlusal problems manifest on the weakest link. If it’s the periodontal tissues, it shows up as a periodontal problem. If it is the muscle/joint, it shows up as TMD. If it’s the tooth, it shows up as a pulpitis or pulp necrosis or perhaps even just a slight apical periodontitis without detectable pulpal involvement.
This hypothesis also explains why an old, previously asymptomatic tooth acts up when a new crown is placed as suggested above; the broken crown that had “self-adjusted” the occlusal disharmony is now hitting in function, and the inflammation kicks up, and the patient is back for occlusal adjustment after occlusal adjustment. While this problem can happen with any restorative material, we believe it is worse with zirconia—much worse!
Also, as a result of these observations, many clinicians in the Four Corners area of Colorado have been placing gold as the definitive restoration on dental implants for many years now—initially, just out of light centric. However, teeth wear and shift and drift, and 5 to 10 years later, we see these very cases with marked faceting on the gold. How did that happen? Where would those forces have gone if they were not to wear the gold? What is to be done about it?
The Problems With Hypothesis Formation From Observational Data
It is universally accepted that cigarette smoking causes lung cancer or, more precisely, is associated with an increased risk for lung cancer. However, this consensus did not occur without considerable controversy. Sir Ronald Fisher, father of the modern statistics, the p-Value, t-test and author of Statistical Methods for Research Workers, didn’t think that cigarette smoking caused lung cancer and wrote extensively on the topic. In Smoking: The Cancer Controversy. Some Attempts to Assess the Evidence, he notes the famous phrase that “correlation does not imply causation.” In Nature in 1958, Fisher writes:
The curious associations with lung cancer found in relation to smoking habits do not, in the minds of some of us, lend themselves easily to the simple conclusion that the products of combustion reaching the surface of the bronchus induce, though after a long interval, the development of a cancer. If, for example, it were possible to infer that smoking cigarettes is a cause of this disease, it would equally be possible to infer on exactly similar grounds that inhaling cigarette smoke was a practice of considerable prophylactic value in preventing the disease, for the practice of inhaling is rarer among patients with cancer of the lung than with others.7
Furthermore, this causal relationship that we now take as established fact has never been demonstrated in a randomized clinical trial, nor will it ever be, as it would be unethical to randomize patients to occlusal disharmony, or smoking to truly establish a causal relationship. In an awkward twist of fate, Fisher, a long-time inveterate pipe smoker, died of lung cancer. From an interventional standpoint, we cannot “un-smoker” a 30-pack-year patient with lung cancer and observe the result any more that we can relieve the occlusion on a necrotic tooth and expect the pulp to revitalize. The damage has been done. So, just as we cannot prove that smoking causes lung cancer any more than we can prove that occlusal problems cause endodontic problems or periodontal problems, there are a lot of sick and dead teeth around. One should at least begin to wonder if these issues proposed, at a minimum, lead to increased risk.
Recommendations for Clinicians
Restorative dentists have a long history of adjusting occlusion on mildly symptomatic teeth and having the symptoms resolve. Those patients never present to the endodontist, periodontist, or prosthodontist, as they were managed by conservative measures under the general practitioner’s care. The patients presenting to the specialty office are the ones who
have not been, and are not getting, managed. The careful specialist with a microscope will often note occlusal adjustments on many of these symptomatic cases and may discover a longer, more protracted pain history upon careful questioning. While we have many of these occlusal adjustment cases that have worked, we also have many that have not. Like the 30-pack-year smoker, the damage was already done. From an intention-to-treat standpoint, however, more invasive treatment is always an option of the occlusal adjustment strategy.
A patient with multiple broken porcelain restorations should be a tip for the clinician as to the increased likelihood of parafunctional issues, and the clinician should carefully consider whether or not it is wise to be replacing these broken porcelain restorations with materials like zirconia that are less forgiving to the issues that caused the broken, worn, and chipped restorations in the first place. In those patients, the restorative dentist may want to consider:
• Avoiding sharp cusps and cuspal inclines
• Flattening and narrowing the occlusal table
• Avoiding zirconia and, instead, substituting gold or a softer tooth-colored indirect material
• Carefully checking centric and excursive movements on implants under high magnification at one year, and every other year afterwards
CLOSING COMMENTS
While it is impossible to prove a hypothesis from observational data, we hope that we have at least offered some evidence of the role of occlusion in some of these kinds of problems. In addition, we hope that we have given the general practitioner readers of Dentistry Today something to think about before diagnosing and treatment planning future cases.
Footnotes
1. Miller’s article occurred at a time when Koch was formulating his famous Four Postulates about the causative relationship between a microbe and a disease. Dentists and dentistry took note, and there was a slew of articles over the following decades (including work by Price cited in Root Cause) with this microbial focus on the disease process that has dominated the conversations in both endodontics and periodontics in the decades since publication. In a blog post for dentistrytoday.com, “Poor Logic and Critical Thinking Skills Allow Root Cause to Seem So Believable,” we discuss this issue in more depth, but wish to introduce it here: Price’s idea of abduction from observational data and generating a new hypothesis for our readers’ consideration. Abduction is a form of inference that starts with observational data and then looks for a simple and plausible explanation for the observations. We may think of abductive inference as having uncertainty, inductive inference as having probability, and deductive inferences as certain (if the premises are true).
References
- Clark D, Khademi J. Modern endodontic access and dentin conservation, Part 1. Dent Today. 2009;28:86-94.
- Clark D, Khademi J. Modern endodontic access and dentin conservation, Part 2. Dent Today. 2009;28:86-93
- Khademi JA, Clark D. Incommensurability in endodontics: the role of the endodontic triad. Dent Today. 2016;35:8-10.
- Khademi JA, Trudeau M, Narayn P, et al. Image-guided endodontics: the role of the endodontic triad. Dent Today. 2016;35:94-100.
- Gangrenous tooth-pulps as centers of infection. In: Miller WD. The Micro-Organisms of the Human Mouth. Philadelphia, PA: S.S. White Dental; 1890.
- Buerger S, Spoering A, Gavrish E, et al. Microbial scout hypothesis, stochastic exit from dormancy, and the nature of slow growers. Appl Environ Microbiol. 2012;78:3221-3228.
- Fisher RA. Cancer and smoking. Nature. 1958;182:596.
Dr. Khademi received his DDS from the University of California San Francisco and his certificate in endodontics and did his MS on digital imaging at the University of Iowa. He is in full-time private practice in Durango, Colo, and was an associate clinical professor in the department of maxillofacial imaging at University of Southern California and is an adjunct assistant professor at St. Louis University. He can be reached at jakhademi@gmail.com.
Disclosure: Dr. Khademi reports no disclosures.
Dr. Blue received his DDS from the University of Missouri at Kansas City (UMKC) School of Dentistry and continued his education by completing a 2-year residency in advanced general dentistry. Dr. Blue practiced general dentistry for 2 years in Kansas City before entering specialty training in periodontics at UMKC in 1999. He received his specialty certificate in periodontics in 2001 and has been practicing periodontics in the Durango area since 2002. He can be reached drblue@drmarkblue.com.
Disclosure: Dr. Blue reports no disclosures.
Dr. Robison received his DDS from the University of Minnesota in 2010. He worked as an associate dentist in North Branch, Minn, for 2 years, then entered a 3-year prosthodontic residency program at the University of Tennessee Health Science Center in Memphis. He earned his certificate in prosthodontics and Masters of Dental Science in 2015 and entered private practice in Durango, Colo. His practice is limited to prosthodontics and implant dentistry in the four corners region. He can be reached at drnathanrobison@twinbuttesdental.com.
Disclosure: Dr. Robison reports no disclosures.
Related Articles
Restoratively Driven, Minimally Invasive Endodontics
A Revolutionary Protocol for Endodontic Access
Image-Guided Endodontics: The Role of the Endodontic Triad


