



The success of replanted avulsed teeth depends on strict conformance with the appropriate treatment at each step between the accident site and the final replantation. The “links” in this chain of events include preparation, action at the accident scene, transportation to the dentist, removal from the transportation device, atraumatic treatment, splinting, and endodontic treatment.1,2
Although there is significant research into how best to store teeth at the scene of an accident, there is little research or advice as to how to get them to the dentist’s office undamaged and in a condition that is conducive to reformation and reattachment of the periodontal ligament. The recommendations for the storage and transportation of avulsed teeth stopped somewhere between 1980 and 1983 when milk was recommended as a possible biologic storage medium.
The Save-A-Tooth System
In 1989, the Save-A-Tooth 1.0 (nee Emergency Tooth Preserving System) became commercially available as a superior alternative to milk. Designed to prevent all of the potential damage between the accident and implantation, it addressed each step in the process between those stages. It included Hanks Balanced Salt Solution (HBSS), a protective netting, an atraumatic removal apparatus, and a shatterproof container.
 |
 |
|
Figure 1. Save-a-Tooth 2.0 improved on the first version, but still had several limitations. |
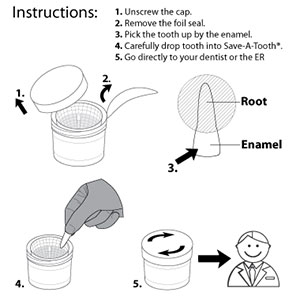
Figure 2. The step by step process for storing and transporting avulsed teeth needs to be followed carefully to ensure successful replantation. |
 |
| Figure 3. The SAT 2.0’s retaining cone-shaped basket, despite its retaining fins, still permitted tooth movement. |
A second iteration, SAT 2.0 (Figure 1), was released in 1994 and corrected many of the difficulties with Save-A-Tooth 1.0. Still, many issues remained. For example, SAT 1.0 was too big and heavy. Although SAT 2.0 reduced the container’s size and weight and, was otherwise very successful, it was still too large to fit easily into first aid kits and other places where emergency gear may be stored, such as glove compartments.
Also, the retrieval part of SAT 2.0 remained confusing (Figure 2). Meanwhile, the Food and Drug Administration’s regulations mandating tamperproof seals changed, making a new seal necessary. The retaining cone-shaped basket, despite its retaining fins, still permitted tooth movement (Figure 3). And, under certain circumstances, such as increased air pressure in airplanes, the tamper-proof seal wasn’t strong. New airline regulations required a more secure seal that conformed with Transportation Security Administration standards.
Save-A-Tooth 3.0 addresses these and other flaws. SAT 1.0 was designed to handle up to 10 teeth, though nearly all emergencies only required storage for four or fewer teeth. SAT 3.0 is a third the size of its predecessors, allowing it to fit into first aid kits easily (Figures 4 and 5).
 |
 |
| Figures 4 and 5. SAT 3.0 is a third the size of its predecessors, allowing it to fit into first aid kits easily. |
 |
 |
 |
| Figures 6, 7, and 8. SAT 2.0 needed to be flipped before the tooth could be removed from the cap. |
Also, the tamperproof seal on SAT 1.0 and SAT 2.0 would sometimes leak with rough handling. SAT 3.0 is 100% leak-free because its closure mechanism acts as a leak-proof seal while also making the device tamperproof.
When removing avulsed teeth from SAT 2.0, the cap had to be placed over the removed basket. These parts then had to be held together and the unit had to be flipped to allow the teeth to fall atraumatically onto the soft sponge so they could be picked up by the enamel (Figures 6, 7, 8).
SAT 3.0 has an easier retention and retrieval system. Each tooth now is held gently but securely by soft, flexible slats (Figure 9), unlike SAT 2.0, which crowded all of the teeth together and separated them only by small plastic fins (Figure 10). Also, with SAT 3.0, the enamel of each tooth sticks up out of the holder and is easily grasped by the fingers or forceps. The roots of the teeth remain bathed in HBSS until removed for replantation.
If the teeth are immature, several drops or granules of doxycycline can be dropped into the HBSS to kill bacteria at the root apex and improve the chances of revascularization following replantation.2,3,4,5 However, recent research has challenged the use of doxycycline to increase revascularization.6
If a tooth does not fit during its reinsertion because the facial bone plate has been crushed or if there is debris in the socket, the tooth can be replaced back in the HBSS in the container while the socket is manipulated to permit a traumatic replantation. The cells are revitalized with the nutrients in the HBSS.7,8 Once the bone is pushed back in place and/or the debris removed, the tooth can be retried in the socket.
 |
 |
| Figure 9. SAT 3.0 has an easier retention and retrieval system. Each tooth now is held gently but securely by soft, flexible slats. | Figure 10. SAT 2.0 crowded all of the teeth together and separated them only by small plastic fins. |
 |
 |
| Figure 11. Tissues never should be used as a storage or transport modality for avulsed teeth. | Figure 12. When teeth fall on the ground, debris lodges in the wet ligament. |
 |
| Figure 13. Teeth that are carried in a glass of milk, water, or even sterile saline are difficult to see because the debris cloudies the fluid. |
Plus, SAT 3.0’s container offers greater resistance to shattering due to its more flexible plastic. It also absorbs side-wall blows, so ligament cells aren’t damaged. Inside SAT 3.0, the fins now simulate a normal socket and hold the teeth gently. The natural motion of carrying SAT 3.0 to the dentist, atraumatically, washes off all of the debris, which sinks to the bottom and goes through the holes there.
Additionally, an improved mixing technique for the HBSS creates a smaller bioburden, reducing the amount of radiation needed to sterilize the internal contents. Less radiation means there is less caramelization of the glucose, making more glucose available for metabolism. Further improvements include, the new mechanical seal, which is stronger and less likely to fail than the previous foil seal and makes placement easier to get into the container. And, the sponge has been eliminated as a landing area.
Previous and Current Recommendations
Nearly all textbooks and other pertinent literature recommend picking avulsed teeth up by the enamel while scrupulously avoiding touching the root surface during retrieval.8,9,10 But then what? Discussions of the treatment of avulsed teeth lack advice or direction for all of the steps between holding the enamel and replantation, aside from the choice of storage fluids and what kind of transport modalities not to use such as tissues (Figure 11).
For example, according to the International Association for Dental Traumatology, “The tooth can also be transported in the mouth, keeping it between the molars and the inside of the cheek but not in children.” This advice, from the most important source of dental trauma information, exemplifies this lack of specific direction.10
When observers at the scene of an emergency see teeth on the ground, they have to pick them up by the enamel and look around for a suitable vehicle and biologic fluid. But if there are three avulsed teeth, how does one hold all of them by the enamel?
Also, the period for finding a suitable vehicle and biologic fluid is severely limited to 15 to 60 minutes.11,12,13 After 60 minutes, the cells, exposed to the air and having depleted their stored metabolites, begin to die. The observer stands there holding the enamel of the teeth while the cells of the ligament die. Placing the teeth in milk after 60 minutes does very little good to replace the lost cell metabolites.
So, unless the teeth are replanted immediately where they were avulsed or unless there is an emergency optimal storage device that can safely transport teeth at the scene of the accident, they are more likely to resorb following replantation. They are especially likely to fail in specific situations. For instance, when a patient in an automobile accident has more serious injuries that require prior attention, avulsed teeth will be ignored unless there’s a storage device at the scene to put them into.
The lack of education among all first aid caregivers and other professionals about the methodology for storing and preserving avulsed teeth has been shown to be a big factor in the large failure rate.11,12,13,14,15 But while this lack of education is a major factor, the lack of supportive armamentarium at the scene of the accident is equally as important. Knowing what to do is useless without the right tools to do it.
The transportation of avulsed teeth to the dentist requires a device that is constructed specifically to preserve, protect, and renew the metabolites and sugars that are necessary for them to continue to metabolize until they are successfully replanted. Teeth that are protected this way can demonstrate more than 90% success in reattachment without significant resorption following replantation.16
Yet there are many potential problems at each step on the path from the accident scene to the dentist. At the accident scene, teeth may be mishandled. There might not be a biologic fluid environment or an atraumatic transport system. People on the scene might not know what to do, or they may be unwilling to help. More serious injuries may need to be treated first. Or, unsafe transportation vessels such as handkerchiefs, tissues, an open glass, plastic wrap, or even the mouth may be used.
What to Do
When teeth fall on the ground (Figure 12), debris lodges in the wet ligament. Since the ligament can’t be touched, care must be taken in cleaning it. Rinsing the tooth in water can damage it because the osmolality is so low. And, because the tooth is slippery, the tooth may be hard to hold when doing so. Instead, avulsed teeth need to be gently washed with a biologic solution.
The process of removing avulsed teeth from the transport vehicle also is more difficult than it seems. Teeth that are carried in a glass of milk, water, or even sterile saline are difficult to see because the debris cloudies the fluid (Figure 13). Getting the teeth out of this solution without crushing the ligament, then, can be difficult and may cause more damage.
In these cases, dentists must grab the teeth blindly with their forceps. Or, if the solution is suctioned out to leave the teeth behind, there may be potential problems with reinsertion. Spilling the fluid carefully while hoping that the teeth won’t slide out from between slippery fingers and onto the floor is challenging as well.
Reinsertion problems may follow, too. If the tooth doesn’t fit in the socket, it will need to be put back into a biologic solution. HBSS would be the best option. But if the transport fluid has been spilled or suctioned out, there would be no medium left for storing the tooth while the socket is modified. Even with a clear solution, dentists still need to grasp the tooth with their forceps, thus, increasing the chance of crushing the PDL.
Accident scenes have several inherent problems too. There is never any armamentarium at an accident scene. For example, adhesive tape and splints are never found just lying around on a football field. All emergency supplies must be brought to the accident scene and able to support every possible accident and be available during every athletic or recreational activity.
Also, consider how some situations may be life threatening. People who are severely allergic to bee stings must have ready access to EpiPens or similar devices. If an EpiPen isn’t available when necessary, the person who has been stung may die.
A similar situation occurs with avulsed teeth. If the tooth is not placed in a biologic storage medium within 60 minutes, the periodontal ligament cells and underlying pre-cementum layer will necrose and lead to progressive root resorption.17,18,19
Optimal storage devices may be overlooked when stocking emergency supplies, but they are available online at amazon.com as well as in dental, athletic training, and school supply catalogs. Claiming that they aren’t readily available would be professionally irresponsible.
Success requires the most biologic treatment at every link in the chain. Like every chain, it is only as strong as its weakest link. If avulsed teeth are brought to an emergency room and no optimal storage devices are there, the periodontal ligament cells will necrose while the patient is waiting for the oral surgeon or other dentist on call to arrive. Or, if the teeth are stored in a damaging milk solution, the results will be poor.
When evaluating the entire scope of the treatment of avulsed teeth, the only conclusion that can be drawn is that there has been a lack of critical insight and recommendations of what is necessary for greater success in implantation. This begins with a lack of education about the biology and treatment of avulsed teeth in dental schools, dental hygiene programs, EMT programs, school nurse programs, medical school, and other health programs.
Summary
For the last 37 years, the treatment of avulsed teeth has focused on the storage solution. Many storage solutions have been tried, ranging from egg whites to medical research fluids.19,20,21 Although some of these have been shown to be compatible with avulsed teeth, the real problem with all of those tested is the same. None of them are ever available at the scene of the accident. Although an egg white may be able to support periodontal ligaments, keeping egg whites available in an ambulance on a daily basis is impractical.
Optimal storage systems are needed at the scene of the accident. These systems need to be able to store, protect, and transport all avulsed teeth, for as long as necessary, to a professional who has the knowledge and equipment to replant them in a biologic fashion. Just as all other emergency medical supplies must be brought to the scene of the accident, optimal storage devices must be a requirement for all first aid kits and emergency vehicles.
Save-A-Tooth 3.0 serves this purpose well. To advance this mission, the SAT system has been redesigned into a new, smaller, more functional, and more effective avulsed tooth preservation and transportation system that can easily fit unto a first aid kit, glove compartment, athletic training bag, or home first aid supplies.
Given the proven benefit of having the most biologic armamentarium at the scene of any accident, all dental organizations should recommend having optimal saving devices wherever people, especially children, are active. Although some teeth are avulsed near home, most are avulsed at locations distant from there. Just as dentists recommend tooth brushing and flossing every day to prevent decay and periodontal disease, they should recommend the optimum treatment for the most serious emergency that will confront most dentists.
References
1. Krasner P. Preventive traumatology. Inside Dentistry. 2012;8:2-7
2. Krasner P. Dental traumatology. Inside Dental Assisting. 2012;5/6:10-16.
3. Krasner PR, Rankow HJ, Ehrenreich A. Apparatus for storing and transporting traumatically avulsed teeth. Compendium. 1989;10:232-238.
4. Cvek M, Cleaton-Jones P, Austin J, et al. Effect of topical application of doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisors. Endod Dent Traumatol. 1990;6:170-176.
5. Trope M. Avulsion of permanent teeth: theory to practice. Dent Traumatol. 2011;27:281-294.
6. Tsilingaridis G, Malmgren B, Skutberg C, et al. The effect of topical treatment with doxycycline compared to saline on 66 avulsed permanent teeth—a retrospective case-control study. Dent Traumatol.2015;31:171-176.
7. Matsson L, Andreasen J, Cvek M, et al. Ankylosis of experimentally reimplanted teeth related to extra-alveolar period and storage environment. Pediatr Dent. 1982;4:327-329.
8. Krasner P, Rankow HJ. New philosophy for the treatment of avulsed teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:616-623.
9. Trope M. Traumatic injuries. In: Cohen S. Pathways of the Pulp. 11th ed. Elvesier; 2015:636-637.
10. International Association of Dental Traumatology. https://www.iadt-dentaltrauma.org/. http://onlinelibrary.wiley.com/doi/10.1111/j.1600-9657.2012.01125.x/full
11. Andreasen JO, Hjørting-Hansen E. Replantation of teeth. I. Radiographic and clinical study of 110 human teeth replanted after accidental loss. Acta Odontol Scand. 1966;24:263-286.
12. Andersson L, Bodin I. Avulsed human teeth replanted within 15 minutes: a long-term clinical follow-up study. Endod Dent Traumatol. 1990;6:37-42.
13. Emerich K, Kaczmarek J. First aid for dental trauma caused by sports activities: state of knowledge, treatment and prevention. Sports Med. 2010;40:361-366.
14. Oleszkiewicz I, Emerich K. How to proceed in case of tooth avulsion: state of student knowledge. Eur J Paediatr Dent. 2015;16:103-106.
15. Mori GG, de Mendonça Janjácomo DM, Castilho LR, et al. Evaluating the knowledge of sports participants regarding dental emergency procedures. Dent Traumatol. 2009;25:305-308.
16. Krasner P, Person P. Preserving avulsed teeth for replantation. J Am Dent Assoc. 1992;123:80-88.
17. Andreasen JO. Effect of extra-alveolar period and storage media upon periodontal and pulpal healing after replantation of mature permanent incisors in monkeys. Int J Oral Surg. 1981;10:43-53.
18. Lindskog S, Pierce AM, Blömlof L, et al. The role of the necrotic periodontal membrane in cementum resorption and ankylosis. Endod Dent Traumatol. 1985;1:96-101.
19. Andreasen JO. A time-related study of periodontal healing and root resorption activity after replantation of mature permanent incisors in monkeys. Swed Dent J. 1980;4:101-110.
20. Ashkenazi M, Sarnat H, Keila S. In vitro viability, mitogenicity and clonogenic capacity of periodontal ligament cells after storage in six different media. Endod Dent Traumatol. 1999;15:149-156.
21. Poi WR, Sonoda CK, Martins CM, et al. Storage media for avulsed teeth: a literature review. Braz Dent J. 2013;24:437-445.
Dr. Krasner is a professor of dentistry at Temple University School of Dentistry. He is the author of more than 80 dental articles on treatment of avulsed teeth, stem cells, endodontic surgery, and pulp chamber floor anatomy. He also is a diplomate of the American Board of Endodontics. He was in private practice of endodontics for 35 years and has lectured extensively on the location of root canal orifices based on the laws of pulp chamber floor anatomy. He can be reached at endsurg@comcast.net.
Related Articles
Dental Offices Need Medical Emergency Preparedness Standards
Traumatic Dental Injuries: Emergency Assessment and Treatment
Exploding E-Cigarette Causes Mouth Injuries







