


The case in Figure 1 is a dramatic example of 3 massive changes that have occurred in the field of endodontics—rotary negotiation of virgin root canals; smaller shapes, fewer files; and the irrigation reboot. Let’s take a look at these changes.
Rotary Negotiation of Virgin Root Canals
Since the beginning of the rotary file revolution, it has been taken as gospel that handpiece-driven files are good for shaping, but only hand instruments are capable of successfully “scouting” through virgin root canals. This turns out not to be true, just as it wasn’t true back in the Sargenti days when we thought anybody who put an endodontic file in a handpiece was a bad dentist.
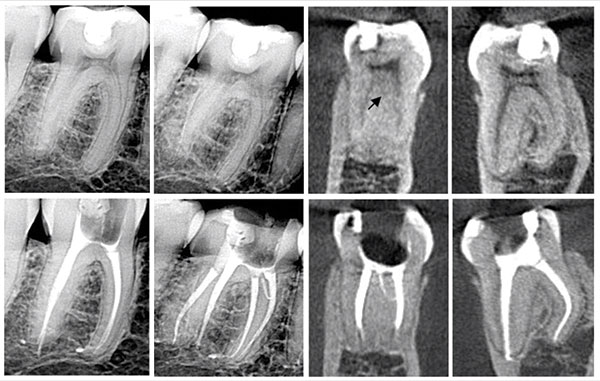 |
| Figure 1. Lower second molar with a distal root that looks out of focus until a side view reveals 2 separate roots, including a conventional distal root and the dreaded disto-lingual root. Traverse Files (Kerr Endodontics) were able to negotiate around even the DL canal with a 90° mid-root bend. In this case, the MB, ML, and DL canals were completely instrumented with a single 13-.06 Traverse File. Note the mid-mesial canal that joins the primary ML canal mid-root. |
Concerns about blocking, ledging, and file breakage have dictated that at least a No. 08 or No. 10 K-file be negotiated to length and beyond before any handpiece-driven file is used to the terminus. This reflects the ubiquitous misunderstanding of what hand files do at the ends of root canals in the first stages of instrumentation. K-files used in these early apps remove very little of the junk in canals. They can break up pulp tissue so it can be irrigated out with a cannula, but they actually increase the volume of debris in canals as dentin is cut off of canal walls and mixed with particulated pulp.
One of the greatest advantages of rotary files is that they auger debris from canals. To me, this is more important than the efficiencies gained by handpiece-driven files. Why? Because I am seeing the majority of US undergraduate endo directors choose reciprocating files for their students on the promise that they will have fewer file separations in the undergraduate clinic. I’ve been on the undergraduate clinical floor of several universities, and nearly every student I have worked with was blocked out 2.0 mm from length in the canals they cut with reciprocating files, wondering why they couldn’t fit a cone to length.
Before rotary files, we could only use one or 2 instruments before we had to thread a patency file to and through the terminus to break up the collected debris so it could be irrigated out of the canal. The day I changed to rotary shaping, that problem was solved—it was no longer necessary to get patent or irrigate between files used. Like most of my peers, it took me a year of using patency files and irrigating between files with this new procedure before I finally realized that there was never anything left in the canal by the rotating files. This functional characteristic of rotary files is why using them as the first instrument to length is not only safe, but (designed effectively) they are safer than hand files in most canals.
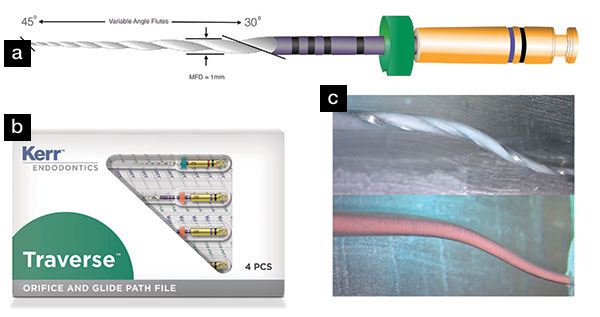 |
| Figure 2a. The 13-.06 Traverse Rotary Negotiating File, with its tip having a 0.13-mm diameter, is smaller than nearly all small molar canal termini. It acts as a passive pilot guide during initial negotiating procedures, threading through apical pulp stumps, pulling them into the flute spaces and out of the canal. Figure 2b. Traverse Rotary Negotiating Files are the first rotary instruments designed to negotiate virgin canals without using any hand K-files beforehand. They are available in 13-.06 and 18-.06 sizes (21, 25, and 31 mm), with an associated 17-mm 25-.08 orifice widener. Figure 2c. A single 13-.06 Traverse File has negotiated and cut to the full shape in an S-shaped plastic block, and an Autofit GP master cone is seen binding exactly and only at its tip. Because Traverse Files have a maximum flute diameter of 1.0 mm, Autofit points are used as they have parallel shank diameters of 0.9 mm. |
 |
| Figure 3a. Lower molar with a 110° kink in the distal canal and an S-curved mesial canal that exited the root at 90°. All 3 of these canals were negotiated with Traverse rotary negotiation files. Figure 3b. Note the absence of any dings or ledging in this grainy but close-up view. Some impediments can be traversed by rotary negotiation files because they have the ability to bump around impediments that would engage an unbent K-file, inviting a ledge. |
It was a surprise to me, but it turns out that blockage, ledging, and breakage occur less often when rotary files are used as the first instrument to length than they do with hand file negotiation; this assumes that instrument design features of the files used have been optimized for this function. What design features are critical for rotary negotiation files? The most important is making them with an open blade angle at the shank end that transitions into tighter angles as the tip of the instrument is approached (Figure 2). This adds strength at the tip of the file and cutting ability at its shank end. The variance of this angle also encourages debris to move up the shank of the file, which is the reason I have never had an apical blockage in 2 years of testing.
The tips of traverse files are tumbled in production to ensure they translate around serious curvatures without ledging, as seen in Figure 3 and the case in Figure 4. The disto-lingual canal in the case shown in Figure 3 had a 90° mid-root kink, and the mesial canals had acute multi-planar curvatures, yet there was no sign of ledging in any of these canals after they were initially negotiated with rotary files. As described in a previous Dentistry Today article about 3% to 8% of canals have impediments that will not allow unbent hand files to get around them, but some of these will allow a rotary file of the right tip geometry to glide around significant canal curvatures.
Smaller Shapes, Fewer Files
Disintermediation can be defined as the removal of an inefficient part of a procedure or business. An example is Uber disintermediating the taxicab.
In endodontics, EdgeEndo gets first credit for disintermediating the entire endodontic file market by driving the price for NiTi files down by half.
Second place in disrupting the endodontic file market goes to endodontists matriculated after 2000, who are seriously concerned about overcutting tooth structure, as they must pitch the case that teeth treated with RCT are as durable as titanium implant fixtures, a drum I have been beating for 30 years. We just don’t need, nor do we want to use, as many files in a canal as we have in the past. More files equal bigger shapes. Files without conservative maximum flute diameters (MFD) are also to be avoided as any file that cuts a larger cervical shape than 1.0 mm is needlessly weakening root structure. Mostly, it’s funny to see all the still-expensive files on the market claiming to be the only file needed when it says in their instructions to begin with hand files.
If you pay attention to your gauging instruments, you will find that many small molar canals can be shaped with just a single ten-dollar 13-.06 Traverse File (Kerr Endodontics). The MB1, MB2, and DB canals in the case in Figure 4 are examples. The disto-lingual root shown in Figure 1 was shaped with a single 13-.06 Traverse File despite its 90° mid-root bend.
 |
| Figure 4. An upper molar treated recently as a live demonstration (see delabs.com for the recorded demo) with buccal canals that were all completely negotiated and shaped with a 13-.06 Traverse File. Note the large mid-root lateral canal bifurcating from the palatal canal and the MB2 canal—shown best in the CBCT image (right)—that bifurcates from the palatal orifice. |
Remember, we only cut tooth structure in root canals for 2 reasons—to optimize canal shape for irrigation and obturation. The corollary to this is the happy fact that young teeth have perfectly tapered canals, so the treatment plan in these cases is to broach the pulp, irrigate for 40 minutes, and fill (Figure 5).
The Irrigation Reboot
The triad of conventional RCT has always been instrumentation, cleaning, and obturation. Advances in instrumentation and obturation procedures have been tremendous, while the development of better irrigation methods has trailed, relatively speaking. Why has this happened?
1. Sodium hypochlorite costs $5 per gallon and remains the all-time champion of RCT cleaning.
After 100 years of using NaOCl as an RCT irrigant, the activity of this inexpensive solution is still the most effective way to remove biofilms, making it a very creative marketing exercise to convince dentists they should buy a supplemental irrigating solution when the directions for use say to use it with NaOCl. That’s impressive. One of these fake cleaning solutions was never sold in Europe because the CE regulations require evidence of efficacy, unlike the FDA’s rules.
Fortunately, in 2010, a new high-tech venture was formed, $50 million dollars was spent to develop a better way to clean root canals, and it’s now an entirely different game (Figure 6). However, even with GentleWave (Sonendo) activation, the hypochlorite shot through this device at 6,000 psi still requires a certain amount of time to clean all the pulp tissue from wide lateral isthmus regions of complex canals (see “GentleWave in Isthmus Research Model” at delendo.com) (Figure 7).
 |
| Figure 5. This young central incisor was treated without cutting any dentin in the canal, as it presented with perfect preoperative shape. The access was cut, the canal was cleaned using the multi-sonic GentleWave procedure, and it was obturated. Note the lateral canal in the last 1 mm of the primary canal—evidence of ideal cleaning and obturation. (Image courtesy of Dr. Steve Frost.) |
 |
| Figure 6. A recently treated upper molar. The MB2 was not instrumented, it was cleaned multisonically, andthen it was cone fit, and obturated in remarkable detail using the new abbreviated Continuous Wave of Obturation downpack with bioceramic sealer. |
2. We have not correctly deconstructed our irrigation failures.
This is also big a topic to address thoroughly in this short article. However, it can be stated in abbreviated form.
My generation of endos was the one who proved to ourselves, our referring dentists, and our patients that it was not only safe to do RCT in a single visit, it was actually better. We initially worried that if we sealed the case, we couldn’t open it up and drain the pressure if a flareup occurred. What we found was that our flareup rates went down, bringing the first golden age of single-visit RCT.
However, following the advent of rotary instrumentation, endodontists began to see an increase in their one-visit failure rates in cases presenting with severe pulpitis. Ironically, because rotary files reduced the time it took to create ideal shaping outcomes (often reducing it from 30 to 5 minutes), clinicians who were used to obturating immediately after shaping was completed saw an uptick in immediate failures, not realizing that their usual modus operandi needed changing to increase irrigation time after instrumentation was completed.
 |
| Figure 7. A research block with prosciutto captured in the replicated isthmus space between 2 primary canals. This significant challenge to the efficacy of irrigation methods showed that GentleWave multisonic irrigation is capable of digesting the lateral pulp tissue replica trapped in the replicated isthmus space in 7.5 minutes. Images (left to right) show the pulp replica in the research block at 0, 1, 3, 5, and 7.5 minutes. |
 |
| Figure 8. This mandibular molar referred pain all over the patient’s left side, within the endo zone, for 18 months after RCT. Retreatment revealed a mid-mesial canal that had harbored pulp remnants with their own mid-root furcal blood supply, which was undoubtedly the reason this pulp stump was able to retain its vitality over the remarkable time period. Just 30 minutes of irrigation time before the RCT was filled would have saved him from a year and a half of significant pain. |
For the next 15 to 20 years, instead of leaving irrigants in canals for adequate periods of time, some of my most well-intended endo colleagues settled for multi-visit RCT, placing CaOH in root canals for 2 weeks to 8 months, then waiting for PR lesions to disappear before finishing the case. That is so 1955. I experienced these failures like everybody else; however, after I read Markus Haapasalo’s research on the critical effect that time has on irrigation efficacy, I upgraded my irrigation times, continued doing single-visit RCT, and have not seen any immediate failures in severely inflamed cases since then (Figure 8).
3. Root canals are frequently more complex than clinicians realize.
Few clinicians have a clue what is inside the teeth they are treating with RCT. Even those of us who are students of endodontic anatomy don’t know how weird the RCS we have invaded really are until we finish the case. Worse news, is that even then, we don’t know what’s in there because of the limitations of our irrigation procedures. If you don’t clean lateral canal anatomy, you won’t fill it, and if you don’t see it in postoperative radiographs, it is easy to believe that RCS’s are simple and that a molar RCT done in 30 minutes is a good value for patients (Figure 9).
 |
| Figure 9. A maxillary molar with an MB2 canal cleaned with a GentleWave procedure and no preceding or following files. The postoperative imaging shows this canal has at least 3 ladder-rung isthmus connections between it and the MB1, which was instrumented with a single 13-.06 Traverse Rotary Negotiation File. |
CLOSING COMMENTS
Dentists, not surprisingly, treat their ideas and beliefs as possessions, because everything we professionally “know” was earned through painful experience or expensive education. That is why we have such a difficult time changing our minds when new information renders previous clinical understandings obsolete. This is illustrated by the famous bad news joke about dental education: Half of what we were taught will turn out to be wrong, and it’s worse than that because we don’t know which half is wrong. I understand this on a personal level as I now use my older lecture slides that once illustrated ideal access cavity design for examples of what to now avoid.
The other reason we resist forsaking long-held beliefs is because we don’t know exactly why we do all the things we do during RCT. A great example is the over-shaped style of RCT that persists among older endodontists to this day, despite the fact that it is deleterious because it reduces the structural strength of teeth without offering any clinical advantages. Herb Schilder designed his zaftig shaping objectives that became associated with quality endo because his Boston University grads, and those who espoused his viewpoint, did the best endo for those 20 years. The underappreciated fact is that he designed those shapes because all we had at the time were stiff, stainless steel files, and all of the condensation devices we had at the time were rigid.
Fast forward to the endo world we currently live in, where we have NiTi files that limit coronal enlargement and can shape a severely curved root canal system with a single file and we can now 3-dimensionally fill, in 2 seconds, everything we have been able to clean through these very conservatively shaped canal preparations.
This may be breaking news to some readers, but these irrevocable changes have already happened, so here’s the deal: You can let go of outdated concepts or be dragged. Instead of just continuing to do the techniques that you were taught in dental school, consider embracing new conceptual and procedural endo advances. It is an exceptional time to provide RCT services!
Dr. Buchanan lives in Santa Barbara, Calif, where he maintains a practice limited to endo-dontics and implants in the same courtyard as his hands-on training facility, Dental Education Laboratories. He has taught thousands of dentists how to perform state-of-the-art root canal therapy, most often with tools he has invented. He invented 3-D printed tooth and jaw replicas to accelerate hands-on procedural training, profoundly changing dental CE experiences. Dr. Buchanan can be reached at the websites endobuchanan.com, delabs.com, and delendo.com.
Disclosure: Dr. Buchanan reports no disclosures.
Related Articles
Inflection Points in Dental Imaging
A Revolutionary Protocol for Endodontic Access








