


 |
| Figure 1. The CEREC chairside system (Dentsply Sirona). |
Thirty-five years ago, Dr. Werner Moorman, along with an engineer named Marco Brandestini, developed the first CAD/CAM system for dentistry. After developing the hardware for the system, Dr. Moorman, who practiced in Zurich, Switzerland, approached the VITA company, which was in nearby Bad Sakingen, Germany, to develop a block that could be milled from his new CAD/CAM system.
Composite restorations were becoming more popular as the restoration of choice over amalgam for patients who were concerned about aesthetics. However, Dr. Moorman was seeing many failed composites in his practice, as these materials were relatively early in their development. His thought was rather than place direct composite restorations that were subject to polymerization shrinkage and potential leakage at the margins, it would be better to mill inlays manufactured from an all-ceramic material and bond those to the tooth structure. Thus, the CEREC system (Dentsply Sirona) was born and, even though the original CEREC was designed originally to mill inlays from feldspathic ceramic blocks, its indications grew over time to fabricate all types of restorations on virtually any tooth (Figure 1).
Early on, adoption of the technology was limited. This was partly due to limitations in clinical indications and, in the author’s opinion, also to the lack of available material options. There were so few CEREC users that companies had no economic incentive to invest in developing further block technologies/materials.
For the first 15 years or so, the VITA Mark II block (Figure 2) was the only one available for CEREC, regardless of the clinical needs that presented. Being a feldspathic ceramic, clinicians were hesitant to use the Mark II blocks in high-stress areas such as molars. Gold; porcelain-fused-to-metal; and, more recently, lithium disilicate and zirconia have been the materials of choice for posterior teeth for the vast majority of clinicians. These materials initially were not available for the CEREC system with full-contour (monolithic) zirconia, having been introduced only recently as another viable option to use for one-visit chairside milling. Today, virtually any class of material is available to mill chairside with the CEREC system. Clinicians are no longer limited to weaker feldspathic blocks, which are more suitable for anterior restorations.
Due to the large increase in the number of CEREC users, manufacturers have been investing heavily into block technology, introducing a multitude of dental materials to satisfy virtually all clinical situations. In this article, we will explore the various classes of dental materials currently available to mill chairside using the CEREC system. The blocks can be broken up into the following categories:
- Anterior aesthetic high-glass porcelain blocks
- Partial- and full-coverage resin-based blocks
- Posterior high-strength, all-ceramic full-coverage blocks
- Implant blocks
- Temporary blocks (for milling provisional restorations)
While this list is accurate as of the publication date, know that as the user base for all CAD/CAM systems grows, manufacturers are regularly releasing new materials for use.
Anterior Aesthetic High-Glass Porcelain Blocks
The anterior aesthetic high-glass porcelain blocks that are currently available are best used in situations that require optimal aesthetics. It should be noted that what clinicians gain in aesthetics with these materials, they give up in strength. Typically, these blocks have a biaxial flexural strength (as tested on the bench) in the 150 MPa range. To put this into perspective, zirconia has a strength in the 1,000-MPa range, and lithium disilicate (such as IPS e.max [Ivoclar Vivadent]) is in the 500-MPa range. The blocks that we will discuss in this section contain the Mark II family of blocks (VITA), which includes both monochromatic and polychromatic blocks as well as IPS Empress (Ivoclar Vivadent) block options—which also include polychromatic and monochromatic blocks—and, finally, the GC Initial Blocks (GC America) (Figure 3).
These high-glass blocks, due to their small particle size and availability in a multilayer format, are the primary choice for the author in the anterior zone. (Note: GC Initial blocks are only available as of this writing as a monochromatic block.) Strength is not the primary characteristic of the high-glass blocks, but strength is usually not a primary concern for most clinicians when working in the anterior region. The author’s recommendation is that these blocks be used in premolars forward (anteriorly) for crowns and veneers. Their small particle size and the ability to position the restoration within the block (in the case of the multilayered options) allow clinicians to achieve optimal aesthetic outcomes (Figure 4).
The software allows the user to position the restoration within the block if he or she wants more or less translucency. In this way, the restoration can be customized based upon the age of the patient. A young patient may need more translucency on the incisal edge, whereas an older patient may not require as much translucency. While the physical properties of these blocks are ideal for anterior restorations, their relative lack of strength, when compared to high-strength ceramic blocks, makes them a less-than-ideal candidate for posterior teeth. It should be noted that early adopters of the CEREC system only had these blocks available during the system’s infancy.
 |
Partial- and Full-Coverage Resin-Based Blocks
These blocks, like the high-glass porcelain blocks, are not known for their high strength. However, due to their resin component, there is some flexibility exhibited in the material. Essentially, the restorations fabricated from these blocks, when used in the proper clinical settings, act with a “bend-but-don’t-break” characteristic. This category of blocks has 2 main types (Figure 5). The first type is a resin-based, zirconia-reinforced nano-ceramic block (such as LAVA Ultimate [3M] and CERASMART [GC America]). The second is a hybrid ceramic, VITA ENAMIC (VITA North America). Even though these blocks contain both a resin and ceramic component, they are now classified by the ADA as ceramic materials.
LAVA Ultimate blocks are indicated for partial-coverage restorations and not full-coverage ones. A higher than desired de-bond rate was noted and documented during full-coverage use of this material. Likely, this may have been due to one of the features (flexibility) that actually makes the blocks ideal for intracoronal use. While the flex in the material is acceptable as the material bends with the tooth under load for partial-coverage restorations, it is an unacceptable characteristic for full-coverage crowns. Due to lack of tooth support, the retention of the material may be compromised, as restorative retention relies heavily on the chemical bond achieved to the milled composite.
CERASMART is indicated for partial- and full-coverage restorations. (Note: A new resin-based nano-ceramic block, BRILLIANT Crios [COLTENE], as of this publication, is undergoing final release in the United States.)
The author’s preference is to use either of these resin-based nano-ceramic blocks for partial-coverage restorations only. These materials, due to their inherent flexibility, are ideal for intracoronal restorations (inlays/onlays). One must realize that the chemical bond is more technique sensitive to achieve with resin blocks than with ceramic blocks. The resin is more highly polymerized, which makes bonding more challenging. When bonding the nano ceramics, micro etching the material is recommended with 50 µm aluminum oxide particles, followed by treating the etched surface with silane or a universal primer (such as Monobond Plus [Ivoclar Vivadent]).
The other type of material in the resin-based block category, as previously mentioned, is VITA ENAMIC (Figure 6). While the author uses this unique material in a similar situation as the resin-based nano-ceramic blocks (partial-coverage restorations on molars and premolars), the composition of the ENAMIC block is completely different than the resin-based nano-ceramic blocks described above. VITA ENAMIC is a hybrid ceramic and is composed of a feldspathic block that has been infiltrated with a polymer component. This gives the material the unique characteristic of being able to have the stiffness of a ceramic with the flexibility of a resin. This unique combination of stiffness and flexibility gives the manufacturer the confidence to recommend a 1.0-mm occlusal reduction (material thickness) in the posterior. For most CEREC blocks, the restoration thickness recommendation is 1.5 mm in the central groove. Due to the high-ceramic content of the material, to prepare VITA ENAMIC for bonding, the manufacturer recommends a 60-second etch with 5% HF acid, followed by a silane treatment. These blocks can be used for inlays and onlays in the posterior, and this is where the strength of these materials really lie.
While both GC and VITA have stated that their particular materials can be used as full-coverage restorations, the author recommends a more retentive preparation and a meticulous bonding technique to ensure success when using the blocks for full-coverage restorations.
Because the resin component of these blocks is already highly polymerized, one major advantage is that the restorations created with them are less susceptible to the potential polymerization shrinkage that may occur with direct composite materials, depending on the material chosen and following a strict placement protocol. (Polymerization shrinkage of the material is one of the reasons that Dr. Moorman saw so many failures in his practice with direct placed composite.) Another advantage of using these materials is that resin-based blocks are a relatively easy material to mill. The material is also kind to the opposing dentition and results in low bur wear on the milling unit, which may be a plus. Finally, in case of restoration damage or unforeseen fracture, repairing resin-based restorations is easier in the mouth than if a ceramic restoration suffered a fracture. Simply micro-etch the restoration in the mouth (with proper isolation), apply silane and a bonding agent, and then do the repair with your composite of choice.
 |
Posterior High-Strength Full-Coverage Blocks
In the author’s opinion, this set of materials has had more of an impact on increasing the number of users who are integrating chairside CAD/CAM into their practices than possibly the improvements in the technology itself, which, when considered, have also been significant. The ability to mill high-strength ceramics means that the clinician does not have to prep differently, or bond/cement the restoration differently, from the usual protocol needed for lab-fabricated restorations.
There are 2 main types of materials that must be considered in the category of posterior high-strength full-coverage blocks: lithium disilicate and zirconia materials.
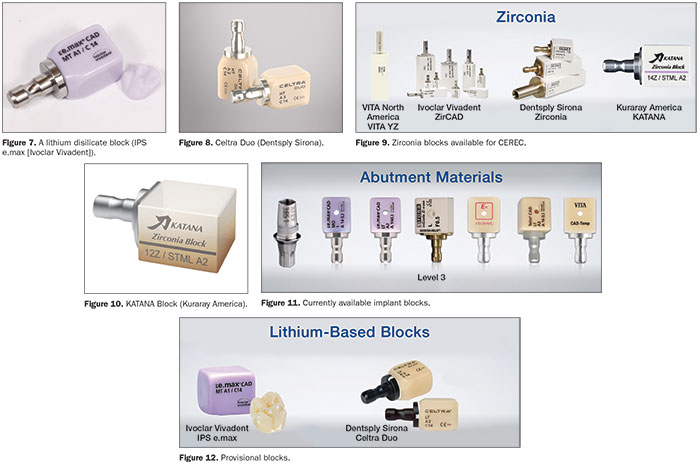
Lithium disilicate (IPS e.max) (Figure 7) was first developed and introduced by Ivoclar Vivadent. IPS e.max has been a popular material used by many clinicians and dental laboratories, including those who employ in-office CAD/CAM technology, for well over a decade. With years of clinical research to support the success of the material, lithium disilicate requires an oven to fire the block to convert the material to its final strength and aesthetics. These blocks are milled in a weaker stage (the unfired block has a slightly purple hue to it) to make it easier to mill the blocks, and the final flexural strength of the material is close to 500 MPa after firing.
This high flexural strength allows the clinician to have a final material thickness of 1.0 mm (minimum posterior occlusal reduction) when using this block.
Another lithium-based block available for the CEREC system is called Celtra Duo (Dentsply Sirona) (Figure 8). Celtra Duo is a pre-crystallized, zirconia-reinforced lithium silicate block that may be polished or fired, depending on the clinical needs of the case. Polishing Celtra Duo yields a flexural strength of roughly 200 MPa, whereas firing the block in an oven will increase the flexural strength up to roughly 400 MPa.
The ability to fabricate zirconia crowns chairside in one visit has been available for the CEREC system since February 2016, with the introduction of the SpeedFire oven from Dentsply Sirona. The SpeedFire oven was the first commercially available oven that allowed the user to sinter zirconia in roughly 15 minutes. Typically, ovens that sintered zirconia required 10 hours (or more) to transform the material from its softer state to its final flexural strength of roughly 1,000 MPa.
Zirconia blocks are available from Dentsply Sirona; Ivoclar Vivadent; VITA; and, more recently, from Kuraray America (Figure 9). The zirconia blocks made by Dentsply Sirona, VITA, and Ivoclar Vivadent have a flexural strength of more than 1,000 MPa. The drawback of this high strength comes at the cost of aesthetics, as these materials are quite opaque and do not provide optimal aesthetics for use in anterior cases.
The KATANA blocks (Kuraray America) (Figure 10) are more translucent and aesthetic, but their strength drops below 800 MPa, which is significantly weaker than the regular high-strength zirconia blocks. The manufacturer recommends a bonded protocol for cementing the KATANA blocks, whereas the blocks from Dentsply Sirona, Ivoclar Vivadent, and VITA may all be traditionally cemented with resin-modified glass ionomer cement. All of these blocks can be fired in the SpeedFire oven, giving the clinician the ability to do a one-visit zirconia appointment.
Implant Blocks
Implant blocks (Figure 11) are available for cement-retained and screw-retained implant restorations, as well as definitive and provisional restorations to be fabricated chairside using the CEREC system. All of the implant blocks work on a similar concept. They are manufactured with a hole in the middle that allows the blocks to be cemented to a titanium base, which is then screwed into the implant.
Ivoclar Vivadent makes IPS e.max blocks that can be used for full-contour restorations and cement-retained restorations. The size 14 MO (medium opacity) block is used for abutments. The medium opacity of the block helps to block out the underlying titanium base. The size 16 LT (low translucency) block can be used for full-contour screw-retained restorations. The Telio CAD (Ivoclar Vivadent) block (described further below) can be used for screw-retained provisional restorations.
The VITA ENAMIC block is manufactured with a hole that can be used for the abutment as well as for the full-contour restoration. VITA North America also makes a block, called CAD-Temp (further described below), that is designed to be used as a screw-retained provisional restoration similar to the Telio CAD material.
Finally, Dentsply Sirona makes zirconia blocks with a hole that can be used as an abutment. A full-contour zirconia block is currently undergoing an FDA approval process.
Temporary Blocks
There are currently 2 options that are available for use as provisional restorations in the United States, the Telio CAD block and the VITA CAD-Temp block (Figure 12). Both come in a 40-mm size, allowing the clinicians to fabricate both individual and multi-unit restorations. When required, the blocks may be modified with a direct composite resin and can serve as long-term provisional blocks.
CLOSING COMMENTS
The purpose of this article was to provide an overall synopsis and a basic categorization of the different CAD/CAM material options available. The different categories and types of blocks have also been presented in an effort to help simplify the indications for the current material choices available to the clinician. There is nothing to say that an IPS e.max or Celtra Duo block cannot be used to mill a partial-coverage onlay or an anterior full-coverage crown. There is no rule that says you cannot use a high-glass porcelain block for a posterior partial-coverage restoration.
In the 35 years since the first dental CAD/CAM system was introduced to the profession, there is no doubt that the increase in the availability and variety of millable materials has led to an increase in the number and type of restorations now being done. There is also little doubt that with advances in hardware/software technologies and in dental material science, clinicians will be provided with even more CAD/CAM treatment options in the future!
Dr. Puri graduated from the University of Southern California School of Dentistry and finished his Advanced Education in General Dentistry residency at the University of Tennessee. He is the Director of CAD/CAM for Spear Education and cerecdoctors.com. Dr. Puri maintains a faculty practice at the Spear Education campus in Scottsdale, Ariz, and has been published in numerous professional journals. He has worked closely with manufacturers over the years as a consultant and served as a CEREC beta tester since 2005. He can be reached at (877) 295-4276, via the website cerecdoctors.com, or via email at sameer@cerecdoctors.com.
Disclosure: Dr. Puri is a principal at Spear Education and cerecdoctors.com.
Related Articles
Entry-Level Milling Unit Returns to the US Market
Study Ranks Chairside CAD/CAM Materials for Toughness
Ivoclar Vivadent Updates IPS e.max Lithium Disilicate








