
INTRODUCTION
For years, Real World Endo has shared with the readers of Dentistry Today clinical techniques and protocols that we have developed and taught to deliver predictable root canal therapy. Our goal has always been to make an otherwise complex and complicated technique simple. In fact, in regard to techniques, our motto has been, “So sophisticated, it’s simple.” However, we realize that we need to teach our philosophy in concert with improved endodontic techniques. Included among these improved techniques are minimally invasive protocols that can benefit the patient. And, as we all know, there is no minimally invasive endodontic technique more relevant than avoiding root canal therapy!
We are all familiar with the old adage, “An ounce of prevention is worth a pound of cure.” Furthermore, in addition to instructing patients about their role in avoiding tooth decay by adopting healthy nutritional habits and improving their oral hygiene, we must also invest time and energy in finding ways to preserve the residual dental pulp of teeth affected by significant caries. Clearly, root canal therapy is a predictable and safe procedure for necrotic teeth and for those pulps diagnosed with irreversible pulpitis, and, over the past 50 years, endodontic therapy has saved millions of teeth for people worldwide.
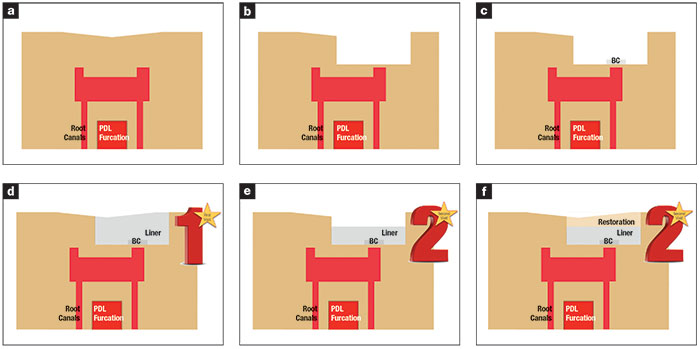 |
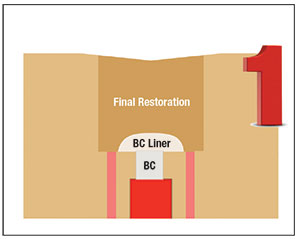
| Figure 1. (a and b) A tooth with reversible pulpitis, after the removal of decay and the proximity or exposure of the pulp. (c) A pure bioceramic, like EndoSequence BC RRM Putty (Brasseler USA), is placed to seal the exposure or cover the area of proximity over the pulp. (d) Since pure bioceramics have a long setting time, the tooth is restored with either a compatible liner material or a provisional during the first visit. (e and f) At the second visit approximately 8 weeks later, when the fate of the pulp is determined and the underlying bioceramic is set, the liner is drilled into for several millimeters to provide a base in order to restore the cavosurface with a definitive material. |
However, although endodontic therapy has been proven to be a safe and effective treatment, we have also learned that the best root canal filling material is indeed a healthy dental pulp! So, first and foremost, our goal should be to preserve pulp vitality whenever possible. To that end, although regenerative endodontics has made strides in regenerating pulp tissue in immature necrotic teeth, we are still years away from a regenerative procedure that can regrow pulp and restore function predictably.
In the meantime, however, an important area that we can successfully manage today with existing technology is the prevention of pulpal necrosis in teeth with reversible pulpitis. This is why obtaining an accurate pulpal diagnosis prior to any clinical treatment, and basing the treatment plan on this specific diagnosis, is an important predictor of successful outcomes. Teeth presenting with caries but with a diagnosis of reversible pulpitis and no specific strategic risk factors are excellent candidates for vital pulp therapy. However, prior to any attempt at vital pulp therapy, we have to establish an accurate pulpal and apical diagnosis that is based on our clinical history and patient evaluation combined with pulp vitality tests and radiographic analysis. When the pulp of a tooth is diagnosed with reversible pulpitis, and it is not of specific strategic importance (eg, the abutment tooth for a long-span bridge where long-term failure may have dire consequences), vital pulp therapy is a good choice instead of root canal therapy. If the pulp testing and history reveals a pulpal diagnosis of irreversible pulpitis, or if the tooth is of significant strategic value, root canal therapy would be the more predictable and preferred approach.
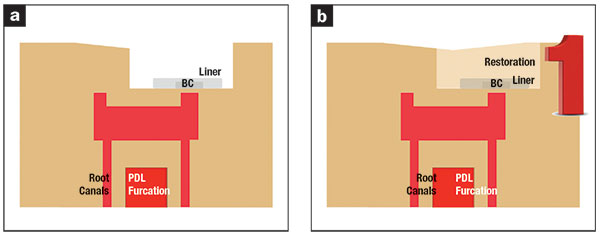 |
| Figure 2. (a) The use of EndoSequence BC Liner (Brasseler USA) allows immediate restoration in a single visit after a bioceramic is used to repair an exposure or pulp capping. A thin layer of BC Liner is placed immediately over the bioceramic layer and light cured, and (b) the final restoration is bonded to it immediately. |
When evaluating whether the treatment of choice should be an indirect pulp cap or a direct pulp cap, the radiographic depth of the decay alone is not adequate enough for proper treatment planning. Instead, the remaining biomechanical strength of the tooth after caries removal, the pulpal and apical diagnoses after pulp vitality testing, and the strategic value of the tooth all must be considered as salient factors when treatment planning a tooth for vital pulp therapy.
Once these factors are assessed and a decision for vital pulp therapy has been made, successful caries removal is another factor of success. After establishing an aseptic field using a rubber dam, caries excavation should be accomplished with both high-speed and low-speed burs. When employing high-speed handpieces, using ample coolant fluids is an important factor for reducing thermomechanical trauma to the pulp during caries removal as well as reducing the odds of pushing microbes and microbial antigens present in dentinal tubules toward the pulp. The entire goal of this treatment is the aseptic and atraumatic removal of caries, and it is critical for success. Depending on the restorative material of choice, many recommendations and different cavity preparation techniques have been described.
 |
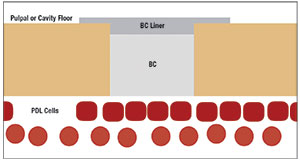 |
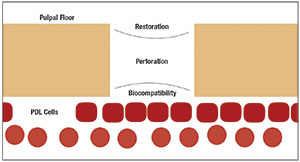
| Figure 3. An area of exposure requires a material with optimal biocompatibility on the cell interface surface and compatibility with the restorative material that covers it. | Figure 4. While a pure bioceramic has the best biocompatibility interface with cells, a layer of BC Liner, which is compatible with pure bioceramics, can act as an interface between the bioceramic and the restorative material inside the cavity preparation. |
 |
| Figure 5. The dual-cure liner material acts as a lid over the unset bioceramic, providing a surface for the restorative material to bond to. |
After atraumatic caries removal, restoration of the cavity is based upon 2 important considerations. Either the material placed is in direct contact with the pulp (direct pulp cap) or is in close proximity to it (indirect pulp cap). The pulp-capping material must have exceptional biocompatibility and should provide an excellent seal from the oral environment. Since this combination has heretofore not been available in one material, dentists have traditionally used liners, followed by placement of a conventional restorative material. Recently, however, pure bioceramic materials have become available that offer improved biocompatibility over traditional liners that contain resins. This new class of calcium phosphate-based bioceramics are hydrophilic and exhibit certain advantages of adhesion, dimensional stability, antimicrobial qualities, and excellent clinical handling properties. Although bioceramics have ideal properties for being close or in contact with pulpal cells, some non-medical grade bioceramics have the disadvantage of a long setting time that can range from one hour to several hours or longer. As a result, the use of these materials for pulp capping or even perforation repair often requires a subsequent visit for definitive restoration of the defect or cavity (Figure 1).
These clinical determinants are why a dual-cure bioceramic liner that has been optimized to interface with a pure bioceramic has been developed by our team with the goal of placing a pure bioceramic adjacent to the pulpal tissue and placing a layer of the dual-cure liner on top of this material. The top bioceramic layer will be used as a light-cured lid to confine and protect the pure bioceramic immediately after placement. The cured liner will then act as a solid surface to bond to the definitive restoration immediately after application of the pure bioceramic material (Figure 2). The cavity can then be restored immediately by bonding to the bioceramic liner.
The important point to understand here is that direct and indirect pulp caps and periodontal perforations represent defects where the utmost biocompatibility is needed on one side of the defect-facing cells and compatibility with the final restoration is required on the other side of the defect (Figure 3). Finally, we have the development of a dual-cure, hydrophilic resin restoration that has been optimized to unleash the power of bioceramics in this domain of preventative endodontics by using a pure bioceramic material against the cells and a bio-ceramic liner that will cover it immediately (Figure 4). This allows the more biocompatible material to be in direct contact with cells and the less biocompatible, resin-containing liner to be in touch with the final restorative material, allowing a final restoration to be placed immediately after repair by using a bioceramic (Figure 5).
The clinical case below demonstrates this concept of combining the biocompatibility offered by a pure bioceramic (EndoSequence BC Sealer HiFlow [Brasseler USA]) with the EndoSequence BC Liner (Brasseler USA) as the covering lid on top of the bioceramic. We refer to this form of sandwich technique as the “Lid Technique,” and we believe it can help improve the efficiency and long-term success of many such procedures where maximal biocompatibility can be achieved in a single-step.
CASE REPORT
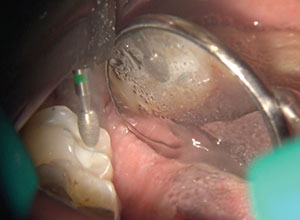
A 35-year-old female patient was referred for endodontic therapy on tooth No. 18, and, after initial caries excavation, deep caries still remained. The tooth was restored with IRM (as a provisional), and the patient was referred for evaluation and possible root canal therapy (Figure 6). Upon consultation, and after gathering pertinent history and doing pulp vitality testing, a pulpal diagnosis of reversible pulpitis and an apical diagnosis of a normal apex were obtained. At this point, the remaining decay was removed under aseptic conditions using a new low-torque, high-speed bur with ample coolant (Figures 7 and 8).
 |
 |
| Figure 6. A symptomatic, previously caries-controlled tooth was referred for root canal therapy with remaining decay. Upon clinical testing, the tooth was determined to have a pulpal diagnosis of reversible pulpitis and an apical diagnosis of normal. | Figure 7. The tooth was adequately isolated with a rubber dam, and the restorative material was removed. |
 |
 |
| Figure 8. The remaining decay was removed completely using a sharp round bur at 40,000 rpm with adequate coolant spray and a light touch. | Figure 9. All decay was removed without exposure. |
 |
 |
| Figure 10. A thin layer of dentin separated the pulp from the cavity preparation, and no exposure was noted. | Figure 11. The premixed bioceramic material was deposited over the depth of the preparation, making sure it did not smear beyond the area of containment, leaving clean dentin surrounding the repair area. |
 |
 |
| Figure 12. BC Liner material was placed gently over the unset bioceramic. | Figure 13. The liner was spread to the rest of the cavity, filling up to the cavosurface margins of the preparation. |
The final cavity was evaluated after all decay was removed without any pulpal exposure (Figures 9 and 10). The cavity was cleaned and damp dried. A thin, homogenous layer of Endo-sequence BC Sealer HiFlow was placed directly against the area adjacent to the pulpal surface (Figure 11). Endosequence BC Liner was then expressed from the automix syringe and gently placed over the unset bioceramic cement to achieve full coverage of the material (Figure 12). At this point, the BC Liner could have been light cured, and a final restoration could have been etched and bonded to it immediately. However, since the patient was to see her restorative dentist for a final restoration, the BC Liner was then used to fill the entire cavity in bulk (Figures 13 and 14), and, after allowing a few seconds for the self-etching material to work, the surface was light cured for a few short seconds with a low-power light source (Figure 15). The rest of the material was allowed to self-set within the next
3 minutes. The rubber dam was removed, and the occlusion was adjusted (Figure 16). The final radiograph shows the more-radiopaque pure bioceramic under the bulk-filled liner (Figure 17).
 |
 |
| Figure 14. The liner was allowed to set and rest for 25 seconds so that the self-etching and bonding could take place. | Figure 15. A low-energy curing light was used for a short 5-second burst to allow the surface of the material to set and allow removal of the rubber dam. The material was left to self-cure for another 2 to 3 minutes for complete curing. |
 |
| Figure 16. The occlusion was evaluated and adjusted. |
 |
 |
| Figure 17. (a and b) Postoperative radiographs show the more-radiopaque bioceramic material against the pulp and the less-radiopaque liner material on top. |
Since the liner is not designed to be a definitive restoration, the patient was reappointed in 8 weeks with her restorative dentist. Once the success of the preventive endodontic procedure has been established at this follow-up visit, the restorative dentist will drill 1.0 to 2.0 mm into the liner and use the rest of it as base to bond a highly polished composite restoration to seal the surface of the cavity.
CLOSING COMMENTS
The introduction of nano-particulate pure bioceramics has established a new era of improved biocompatibility that includes better root repair and vital pulp therapy outcomes that will establish preventive endodontics as a legitimate goal of all endo-restorative procedures. Until recently, the main limitation for the use of pure bioceramics has been their extended setting times.
In this article, we have described a clinical technique that combines a pure bioceramic with a novel dual-cured bioactive resin ionomer that has been optimized to work in conjunction with pure bioceramics. The sandwiched liner material interacts with the final restorative material on one side and the pure bioceramic on the other side. The hydrophilic nature of this liner, combined with its high flexural and compressive strength, makes it the ideal material for coverage over unset bioceramics. This combination will allow single-visit repairs and vital pulp therapy procedures to become more convenient. We are optimistic that further research and development in this area will help improve these preventive clinical techniques in the years to come. Furthermore, we hope that the application of this bioactive liner will encourage the use of endodontic repair and pulp vitality procedures, which, in combination with proper diagnosis and treatment planning, will improve the success rate of preventive endodontics.
Dr. Nasseh received his Master of Medical Science degree and certificate in endodontics from the Harvard School of Dental Medicine in 1997. He received his DDS degree in 1994 from Northwestern University Dental School. He maintains a private endodontic practice in Boston (msendo.com) and holds a staff position in Harvard’s postdoctoral endodontic program. Dr. Nasseh has lectured extensively on such diverse topics as diagnosis, anesthesia and sedation, and microsurgery. He is the endodontic editor for several dental journals and periodicals and is on the clinical advisory board of the Michigan-Pittsburgh-Wyss Center for Regenerative Medicine. He is the CEO and president of Real World Endo (realworldendo.com). He can be reached at anasseh@hsdm.harvard.edu.
Dr. Koch received both her DMD degree and certificate in endodontics from the University of Pennsylvania School of Dental Medicine (Penn Dental). She is also the founder and past director of the Postdoctoral Program in Endodontics and Microsurgery at the Harvard School of Dental Medicine. Following her clinical and academic career, she formed her own successful technology and development company, Real World Endo, of which she was CEO and president. Dr. Koch is the holder of multiple patents, maintains a faculty position in the Department of Endodontics at Penn Dental, and serves as a Senior Fellow with Penn Medicine. She is also a member of the Board of Overseers for Penn Dental and maintains an adjunct faculty position at the Harvard School of Dental Medicine. She can be reached at annelaurenkoch@gmail.com.
Disclosures: Dr. Nasseh is president and CEO of RealWorldEndo and has helped develop Bio-Ceramic Putty and BC Liner products. Dr. Koch is a consultant for Brasseler USA.
Related Articles
Three-Dimensional Anatomic Cleaning and Shaping
Three-Dimensional Instrumentation: The Promise of Minimally Invasive Preparations
Why Do We Do What We Do? A New Standard of Efficiency in Instrumentation and Obturation

