


INTRODUCTION
As a practicing endodontist and a clinical endodontic educator for more than 30 years, the most frequent question I am asked about technique is: “Is it predictable?” While every dentist wants his or her endodontic treatment to be easier, more efficient, simpler, and profitable, in the end, it is predictability that trumps all considerations. As dentists, we are built that way and that’s how we think. We have to do it right. We are a self-selected culture that yearns to be better and to be our best.
Endodontic success rarely depends on a dental lab or whether or not the patient even cleans his or her teeth! Endodontic success does depend on the thoroughness of cleaning, shaping, and 3-D obturation—the classic and time-tested Endodontic Triad. This is where we, the dentists, come in. Predictable endodontic success, therefore, depends on (1) our knowledge of what to do, (2) our skill set in doing what we need to do, and, finally and most essentially, (3) our willingness to do it right. We have a direct relationship to endodontic predictability. If we are careful and do it right, nature does the rest. The purpose of endodontics is to heal lesions of endodontic origin (LEOs) where they exist and prevent LEOs where they do not exist.1-3
When I am asked the question “Rotary vs Reciprocation: How Do I Choose?” my answer is “Rotary and Reciprocation,” because the predictability of both methods is similar; they are just different in sequence, purpose, and motion. The goal of this article is to explore and explain these 3 critical distinctions of Rotary vs Reciprocation so that the clinician is aware of these differences, understands his or her options, and makes the best choice for his or her particular practice and patient needs. This article is an invitation to be self-educated about your best way to produce endodontic preparations that can be easily obturated.
As a disclaimer, please note that I am a co-inventor of ProTaper and WaveOne file systems (Dentsply Sirona Endodontics). As such, I have an internal bias. However, if you take the self-test that I suggest at the end of this article, your choice of Rotary vs Reciprocation will be self-evident, perfectly scientific, and all about your and your patients’ needs. In this clinical article, the examples I use for Rotary vs Reciprocation are ProTaper Gold (PTG) and WaveOne Gold (W1G) (Figures 1 and 2). These are the file systems I helped design and know the most about. You can substitute any rotary brand for my ProTaper Gold distinctions and any reciprocation brand for my WaveOne Gold distinctions. The principles of The Challenge Testing essentially remain the same.
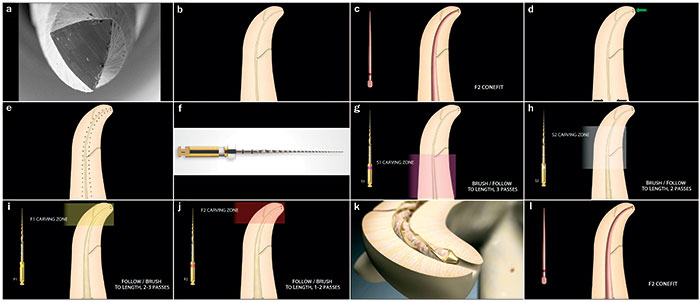 |
| Figure 1. The features, sequence, purpose, and motion of ProTaper Gold (PTG) (Dentsply Sirona Endodontics). (a) Convex triangular “cutting” blades have made Rotary shaping highly efficient, while Gold technology has made shaping safe. (b) Animation of pretreatment image. (c) Starting with the answer—the appropriate gutta-percha conefit is vividly imagined. The most common maximally appropriate shape is produced with the F2 (25/08) Finishing file. (d) Soon-to-be discovered apical constriction width is identified by 2 dots and the anticipated one fifth to one third of the coronal width (nature’s diameters for structurally successful teeth) is also identified by 2 dots. (e) The shaping goal is to smoothly “connect the dots” apically with the dots coronally. (f) The ProGlider mechanical file (Dentsply Sirona Endodontics) may be used to expand the smooth, super-loose No. 10 file Glidepath. (g) The PTG S1 carves away coronal third restrictive dentin from the inside out. (h) The PTG S2 carves away restrictive dentin in the middle third of the canal. The PTG S1 and PTG S2 are used in a Brush/Follow sequence to length. (i) The PTG F1 is used in a follow/brush motion to length. If apical blades are nude of dentin shavings, this is a cue to progress to the next larger size (PTG F2) in order to confirm the apical shape. (j) Dentin-loaded PTG F2 apical flutes prove the apical shaping is complete. (k) An animation image illustrates PTG F2 blades cutting a perfect F2 radicular preparation shape. (l) A successful PTG gutta-percha conefit means the root canal system is ready for 3-D obturation. |
Definitions
Rotary, in the context of this article, refers to mechanical radicular endodontic shaping where the cutting blades function in a continuous clockwise (CW) direction. Put crudely, the motion resembles that of the common drill.4-7
Reciprocation, in the context of this article, refers to mechanical radicular endodontic shaping using unequal bidirectional clockwise/counterclockwise (CW/CCW) directions. Put crudely, the motion resembles that of a Roto-Rooter. The ProMark and X-Smart iQ endodontic motors and handpieces (Dentsply Sirona Endodontics) produce both continuous rotation and reciprocation motions within a single motor (Figure 2l).8-11
Literature
Mechanical rotary and reciprocation articles are abundant in the literature. Using PubMed to search the keyword “ProTaper” yields 912 published studies in the last 10 years. Using PubMed, there are also 19 studies returned from searching the term “ProTaper Gold” within the last 5 years. A search in the Journal of Endodontics from “All Available Dates” reveals 256 articles where “ProTaper” appears in the abstract. A similar search using Google Scholar and the search term “ProTaper AND Dentistry” shows 7,530 results from 2007 to 2017. Similarly, a search using PubMed and keyword “WaveOne” yielded 220 studies in the last 10 years. A search in the Journal of Endodontics from “All Available Dates” shows 75 articles where “WaveOne” appears in the abstract. A search using Google Scholar and the term “WaveOne AND Dentistry” reveals 2,590 results from 2007 to 2017.
Using membership surveys for the past 6 years, I have explored Rotary vs Reciprocation percentage usage among endodontists. Endodontists clearly prefer Rotary vs Reciprocation, but with the introduction of Gold technology, I am observing an increase in both Rotary and Reciprocation among endodontists.12
History
The need to design and create smooth, funnel-shaped radicular preparations was void in clinical technique before the discovery of NiTi mechanical shaping files. Since dentists could not see inside the root canal system, we could not “do and see” simultaneously, unlike other dental preparations. It might be said that in endodontics, “we do it in the dark.” Before mechanical shaping, manual shaping could not provide the smooth, funnel-shaped preparations because of their .02 taper. Manual shaping tends to carve and cut at unpredictable and often undesirable points along the file’s shaft rather than smoothly “connecting the dots” between the minimal apical canal physiologic diameter and the desired coronal canal width, which nature has identified between one fifth and one third of the root width (Figures 1 and 2).
The Moment Before “The Moment”
Every dentist that has ever mechanically shaped a radicular preparation knows and can emotionally recall the feeling of the moment before “The Moment” (Figure 3). What is this moment? Following an unfettered canal access by first removing all coronal dentin triangles with a PTG SX shaping file (Dentsply Sirona Endodontics), for example, and following a confirmed reproducible Glidepath, the moment I am referring to is the very seconds before you ultimately reach length without breaking the file.13-17 In the moment before the Moment, the fear of fracture can take away the joy of endodontics, and, like a self-fulfilling prophecy, sometimes we break the file in spite of our goal to shape with safety. Every endodontic clinician knows the sinking visceral feeling of a broken file. The energy level goes out of the operatory and often can kill the day’s enjoyment level. Since the advent of Gold heat-treated mechanical shaping files, the moment before “The Moment” has completely changed for most practitioners. Gold-heated technology increases flexibility, and improves cyclic fatigue, and is more efficient. The increased efficiency is because the Gold metallurgy, without distortion, snuggles more easily against dentin walls and, therefore, cuts more conservative funnel shapes. In the moment before the Moment, fear turns to fun, concern to confidence, and consternation to control. The positive possibilities of this clinical experience of the moment before the Moment makes it worth taking the “Rotary vs Reciprocation Challenge” at the end of this article and to join the predictable shaping fun.
 |
| Figure 2. The features, sequence, purpose, and motion of WaveOne Gold (W1G) (Dentsply Sirona Endodontics). (a) SEM of W1G, courtesy of Nova Southeastern University Bioscience Research, showing a parallelogram-shaped cross section enabling only 2 points of cutting contact during the file’s unequal bidirectional motion. (b) Pretreatment animation. (c) The imagined conefit before shaping begins. (d) Anticipated apical and coronal preparation widths are identified. (e) Apical and coronal dots are smoothly connected in an imagined preparation shape. (f) After the manual super-loose No. 10 file is used, a GoldGlider (Dentsply Sirona Endodontics) is recommended to expand the Glidepath to more easily accommodate the W1G Primary (25/07) file. (g) The first pass with the W1G shapes the coronal portion of the radicular preparation. (h) The second pass of the W1G Primary cuts the middle third of the prep. (i) Animation of a crown-down W1G preparation. (j) A third pass of W1G finishes the apical prep. (k) The desired shape is confirmed with the matching conefit. (l) ASI’s (Advanced Systems Integration, Englewood, Colo) endodontic cart houses the ProMark motor and, like the X-Smart iQ motor (Dentsply Sirona Endodontics), it can be set for either Rotary or Reciprocation. |
Clinical Distinctions
Rotary: Following a reproducible Glidepath, the clinical technique of Rotary is an “inside out” concept. In the case of PTG, the Shapers specifically cut away restrictive coronal dentin by intentionally, precisely, and progressively brushing away the restrictive dentin in an essentially lateral motion. Think of the Shapers as a brush and not a drill! The Shapers first fit easily within the canal to be shaped and then cut the radicular coronal restrictive preparation by laterally brushing and then removing it. The PTG Finishers produce shapes similar to Reciprocation-produced shapes. However, the technique to create Rotary vs Reciprocation shapes is quite different. In PTG shaping, the radicular dentin preparation relies on the clinician’s commitment to progress through a sequence of Shaping instruments where each instrument’s preparation allows the next Shaper and Finisher to easily fit (Figure 1).
Reciprocation: Following a reproducible Glidepath, the clinical technique of Reciprocation has always been a “crown-down” concept. Where PTG has classically called for one to 4 instruments, one of W1G’s distinctive values is in selecting and using a single file such as Primary, which has similar, though not exact, geometries as PTG Finisher No. 2 (red). Because a single W1G file is being asked to produce a similar predictable conefit as with multiple PTG files, a different skillset is required and is described below (Figure 2).
Sequence
Rotary: After the Glidepath is validated, the color sequence is unmistakable and never varies ( ). The color sequence is the recognizable ISO standard color sequence and is, therefore, easy to remember. No mixing and matching; just follow the color order as the optimal sequential geometries have been researched, calculated, and clinically tested (Figure 1).
Reciprocation: After the Glidepath is validated, the sequence is also unmistakable and even further simplified. The color is usually Red and Red only ( ). The Red (Primary) file is used in a multipass sequence. Restraint and confirming patency are key watchwords during every pass in the multipass sequence, since a single file is replacing the workload of a multiple file sequence, such as Rotary shaping. Irrigation and confirming patency are also recommended with each separate W1G pass in order to prevent blocks, ledges, perforations, and transportations (Figure 2).
 |
| Figure 3. The moment before “The Moment.” Every dentist knows this moment. The Moment refers to the dentist’s fleeting thought right before mechanical files engage the radicular root canal system walls as the file begins to cut its own shape. Until heat treated and improved file geometries such as PTG and W1G, this Moment was filled with concern and fear of breakage. Now with a reproducible Glidepath, proper mechanical directions for use (DFU), new files, and a gentle touch, the moment before the Moment has been changed from fear to energetic confidence and predictability. With confidence, endodontic shaping has truly become fun! |
Purpose
Rotary: PTG S1 (purple) cuts away restrictive dentin in the coronal third, PTG S2 (white) cuts away restrictive dentin in the middle third, and PTG F1 (yellow) carves the perfect shape in the apical third, followed by PTG F2 (red) and PTG F3 (blue) if needed (Figure 1).
Reciprocation: The Primary W1G (which has similar external geometries to PTG F2) cuts the entire length of the radicular preparation using a multipass technique (Figure 2).
Motion
Rotary: Shapers are first gently followed into the existing unrestricted orifice, then withdrawn in a paint-brushing motion, and then followed deeper into the preparation. The mental chant is “Brush and Follow (deeper), Brush and Follow, Brush and Follow” to length. The Shaper file is only removed if the file bogs down with dentin shavings. If this were the situation, it is usually because the file’s blades are loaded with dentin carvings and/or remaining pulp. Remove the file and irrigate with sodium hypochlorite or EDTA. Clean the blades and continue. The Shaper file will now progress easily after each Brushing motion as it had done before (Figure 1).
Once the Shapers have reached desired length, the Finishers prepare the final shape by connecting the dots (Figures 1e and 2e). The Finisher’s motion is in reverse order of the Shapers. The Finisher’s chant is “Follow and Brush (coronally), Follow and Brush, Follow and Brush” to the desired preparation physiologic terminus length. Fit the PTG cone or verifier to confirm the shape.
Reciprocation: Because the crown-down approach with a single file is asking that single file to do the work of 2 or more files, different motions are needed. Also, since a single file is being asked to follow a narrower canal than the file itself, there is a greater possibility of blocking the canal with collagen or “dentin mud” (a mixture of detached necrotic pulp and dentin instrument filings).18 Typically 2 to 6 “passes” are required to reach length. The motion is simple and similar in chant as with Rotary Finishers in PTG technology: “Follow and Brush, Follow and Brush, Follow and Brush” to length. The big difference, however, is that with each “Follow and Brush,” or “pass,” the Reciprocation file should be removed, the file should be cleaned of dentin filings, the canal should be irrigated, patency should be confirmed with the No. 10 manual file, and the canal should be irrigated again. Then proceed with “pass” No. 2 and so on until preparation physiologic terminus length is reached. Fit the W1G cone or Verifier to confirm the shape.
The Greatest Variable
In all of dentistry, the greatest variable is always the clinician. While product and operatory infrastructure play a significant role, the answer to Rotary vs Reciprocation depends mostly on technique, and technique depends on the clinician’s skill, care, and judgment.
Q: How Do I Choose?
A: Take the Challenge
Here is a simple and revealing test for each clinician to determine his or her own preferred “Rotary vs Reciprocation” choice: Call your local dental sales representative (in my case it would be the Dentsply Sirona Endodontics sales representative). Tell him/her you want to do this “challenge” test: Purchase enough Rotary files (PTG in my example) and enough Reciprocation files (W1G in my example) to treat 10 endodontic patients with Rotary and 10 endodontic patients with Reciprocation. You could treat every other patient alternately with Rotary and Reciprocation, or you could treat 10 patients in a row with Rotary and then 10 with Reciprocation. Reverse the order if you prefer. You can use this same telltale test for comparison with your current preferred system. Take good notes about what worked and did not work. Your answer for Rotary vs Reciprocation will be right in front of you!
CLOSING COMMENTS
When properly performed, endodontics is highly productive and fun! Using predictability as your critical benchmark distinction, your own testing will reveal your best choice of “Rotary vs Reciprocation.” The result: clinical confidence, consistency, and control. The marketplace has actually already answered the question of Rotary vs Reciprocation. The market’s answer: “Rotary and Reciprocation.” Those clinicians who have done their own in-house, controlled homework and testing will be happy with their answers. Now it’s your turn!
Albert Einstein did not read this article, but he knew oh so well the value of self-education and self-testing. The following quote from Einstein is the perfect takeaway for this article about using the scientific method to self-discover your answer to the question of Rotary vs Reciprocation: “The only source of knowledge is experience.”
References
- West JD. Finishing: the essence of exceptional endodontics. Dent Today. 2001;20:36-41.
- West JD. How do masters do it? Dent Today. 2012;31:102-107.
- West JD. Endodontic predictability: “What matters?” Dent Today. 2013;32:108-113.
- West JD. Introduction of a new rotary endodontic system: progressively tapering files. Dent Today. 2001;20:50-57.
- West JD. Progressive taper technology: rationale and clinical technique for the new ProTaper Universal system. Dent Today. 2006;25:64-69.
- Ruddle CJ, Machtou P, West JD. Endodontic canal preparation: innovations in glide path management and shaping canals. Dent Today. 2014;33:118-123.
- West JD. Ni-Ti goes gold: “ten clinical distinctions.” Dent Today. 2015;34:66-71.
- West JD. Is the new WaveOne endodontic reciprocation for me? Dental Economics. 2011;101:32-33.
- Kuttler S, West JD. Single file system: “the science of simplicity.” Dent Today. 2012;31:92-95.
- Ruddle CJ. Canal preparation: single-file shaping technique. Dent Today. 2012;31:124-129.
- Ruddle CJ. Single-file shaping technique: achieving a gold-medal result. Dent Today. 2016;35:98-103.
- West JD. New trends in endodontics and treatment planning. Dent Today. 2017;36:64-69.
- West JD. The endodontic Glidepath: “secret to rotary safety.” Dent Today. 2010;29:86-93.
- West JD. Manual versus mechanical endodontic Glidepath. Dent Today. 2011;30:136-140.
- West JD. Glidepath implementation: “return to the beginning.” Dent Today. 2011;30:90-97.
- West JD. The three Fs of predictable endodontics: “finding, following, and finishing.” Dent Today. 2016;35:90-96.
- West JD. Single versus multiple endodontic file use. Dent Today. 2016;35:62-67.
- West JD. Perforations, blocks, ledges, and transportations: overcoming barriers to endodontic finishing. Dent Today. 2005;24:68-73.
Dr. West received his DDS from the University of Washington, where he is an affiliate professor. He earned his MSD in endodontics at the Boston University Henry M. Goldman School of Dental Medicine, where he is a clinical instructor and a member of the Alumni Board and was awarded with the Distinguished Alumni Award. He is the founder and director of the Center for Endodontics in Tacoma, Wash. He also mentors the world’s only stand-alone, 4-day mini-endodontic residency program at the Interdisciplinary Dental Education Academy in San Francisco. He is a Fellow and was the 2009 president of the American Academy of Esthetic Dentistry and the 2010 president of the Academy of Microscope Enhanced Dentistry and is a member of the former Northwest Network for Dental Excellence and the International College of Dentists. He was a 2010 consultant for the ADA Board of Trustees and the ADA Council on Dental Practice. Dr. West is in private endodontic practice in Tacoma. He can be reached via email at the address johnwest@centerforendodontics.com.
Disclosure: Dr. West is a co-inventor of the ProTaper and WaveOne endodontic shaping systems.
Related Articles
Removing the Mystery: Treating Multirooted Teeth








