To say that BOTOX is a popular aesthetic treatment is a vast understatement. Over 21 years has passed since botulinum toxin A (BTX-A) injections (BOTOX) was introduced for use in treating unsightly frown lines between the eyes and the smoothing of facial wrinkles. BOTOX treatments are the most commonly performed minimally invasive cosmetic procedure in North America. There were nearly 2.5 million cosmetic procedures done with BOTOX in 2008, according to the American Society of Aesthetic Plastic Surgery. Women accounted for 92% of the total cosmetic procedures done. BOTOX cosmetic procedures accounted for 24% of all cosmetic procedures done in 2008. Compared to just about any other delivered medication on the market, the safety records of BOTOX treatment is nearly unparalleled.1
|
|
||
|
THE QUICK BOTOX PRIMER
BOTOX is a trade name for botulinum toxin, which comes in the form of a purified protein. BTX-A is the most commonly used form with several thousand articles supporting its use found in the scientific and medical literature. The mechanism of action for BTX-A is really quite simple. It is injected into the facial muscles and, within a few hours, it attaches itself to the nerve endings of the motor muscles, thereby affecting the nerve transmission to these muscles. It takes anywhere from 2 to 10 days to block the nerve transmitters which innervate the muscles into which it was injected. There is no loss of sensory feeling at all during the time that BTX-A is effective. Once these motor nerve endings are interrupted, the muscles cannot contract. When the muscle does not contract, the dynamic motion that causes wrinkles in the skin will then cease. The only reason there are wrinkles in the skin in the first place is because the muscle is moving underneath it, thereby these are called dynamic wrinkles.
Approximately 3 to 10 days after treatment, the skin above these motor muscles becomes nice and smooth. The effects of BOTOX lasts approximately 3 to 4 months depending on various factors including the amount of BTX-A injected, metabolic activity of the patient and lifestyle choices, which may cause the BOTOX treatment not to last as long. When the patient sees the wrinkles reappear, the patient needs retreatment. This is one of the reasons that BOTOX has such an incredible safety record. BTX-A treatment, by its nature, is a temporary treatment and when the treatment effects are gone, they are gone completely. This is a little different than the usual mindset of dentists. We as dentists don’t usually think of our treatments as temporary. From the standpoint of comparing treatments that are temporary in nature, the most common dental treatment that is like BOTOX therapy is teeth whitening. Teeth whitening is a temporary procedure that needs to be refreshed from time-to-time.
FACIAL AESTHETICS
The most common uses for BOTOX is smoothing of the facial wrinkles of the forehead, between the eyes (glabellar region), and around the corners of the eyes (crow’s feet) (Figures 1 to 5). These are the most common cosmetic uses that have put Botox on the aesthetic map.
 |
 |
| Figure 1. A 42-year-old facial pain patient with strong frontalis muscle contraction. |
Figure 2. Dynamic wrinkles associated with the muscle contraction. |
 |
| Figure 3. BOTOX therapy relieves her pain and gives her a great aesthetic result. |
DENTAL USES FOR BOTOX
Now that approximately 7% to 8% of dentists (and growing) in North America are currently providing BOTOX treatment to patients for cosmetic treatment, there are other innovative uses being found for BOTOX in dentistry (private communication, Allergan Corporation). Most dentists are not aware of the substantial benefits that BOTOX has as an adjunctive therapy in dental and cosmetic treatment. BOTOX has useful clinical uses as an adjunct in temporomandibular joint (TMJ) and bruxism cases, even more so for patients with chronic TMJ and facial pain. BOTOX is a muscle relaxer and when given in typically half the dosage used for facial wrinkle smoothing treatment, it can greatly reduce the intensity of the muscle contractions that contribute to TMJ and facial pain and give the patient significant relief. We have all had TMJ patients that have gotten the bruxism appliances, have done full-mouth reconstructions, and are still at wits end in trying to find the right answer that will help them with their facial pain. BOTOX can play a very important role in reducing or eliminating their facial pain.2-5
BOTOX is often used in conjunction with dermal filler therapy as a nonsurgical alternative to high lip-line cases. Figures 6 and 7 describe such a case. This patient has a nice smile with a significantly high lip-line showing on the left side of her mouth when she smiles. The treatment that most dentists have been trained to deliver to these patients would be some kind of periodontal flap surgery. This would include significant osseous reduction through a crown lengthening procedure in order to be able to raise the gingival height to meet the lip-line. The patient would then require crown and bridge therapy to better establish the dental aesthetics. Every dentist knows how aggressive treatment like this would be. I would venture to say that few dentists, if they were the patient, would want to proceed with that kind of aggressive treatment, yet this is what many offer to their patients. With some BOTOX therapy and lip augmentation with dermal fillers, the muscles surrounding the lip are weakened, so they cannot raise the lip as high as before. This has to be done carefully so that the patient maintains full lip competency allowing them to go about their normal activities such as speaking, smiling, puckering, and eating. When done correctly, the patient is not able to raise her lip as high as before to show the gingiva on the left side, but still has the full ability to speak, chew, and kiss.
It is important to be able to offer all of the alternatives to the patient for high lip-line cases. The advantages of the aggressive treatment option of crown lengthening, possible orthodontics, and crown and bridge therapy, are that the results will be long lasting and can be aesthetic. The disadvantages are that the treatment will take a number of appointments, high cost immediately, possible complications of said treatment—including sensitivity, possibly requiring endodontic therapy later on, and necessary retreatment in 10 to 15 years as gingival recession occurs. The advantages of treating cases like the one above with BOTOX and dermal fillers are the close-to-immediate results in one appointment with no removal of any tooth structure. The disadvantages are the needed re-treatment 2 to 3 times a year and the cost associated with that repeated treatment. It makes no difference to me as the clinician which treatment option the patient chooses, but it significantly expands the treatment choices that we now have.
 |
 |
|
Figure 4. Wrinkles around the eyes (crow’s feet) make this patient look older than she really is. |
Figure 5. BOTOX gives her the aesthetic result that she desires. |
 |
 |
|
Figure 6. This patient has an unaesthetic high lip-line on the left side when she smiles. |
Figure 7. Combination therapy of BOTOX and dermal fillers for muscle relaxation and lip augmentation respectively demonstrates a minimally invasive approach of correcting the lip-line and gingival discrepancy. |
A BEAUTIFUL SMILE, NOT JUST BEAUTIFUL TEETH
The above case demonstrates that BOTOX and dermal fillers are as essential to aesthetic dentistry cases as porcelain veneers and composite resins. The soft tissues around the mouth are as important as the color and position of the teeth in determining the patient’s smile. We, as dentists, have become so tooth-centric that we forget that it is very important for the perioral areas to look as good as the teeth. This concept of framing the smile properly is essential in order to perform a complete smile analysis and any associated aesthetic treatment. How many times have you seen an aesthetic dental case involving beautifully restored teeth that are left surrounded by wrinkled and thin lips, and deep nasolabial folds? Perhaps the patient has been given beautiful teeth but not a completed and beautiful smile.
BOTOX IN OTHER ROLES
BOTOX has also been used in other areas of dentistry including retraining muscles during orthodontic therapy. Orthodontically, you can move the teeth all you want, but, if you have strong to severe muscle movement, teeth will relapse, especially in patients with a very strong mentalis muscle. Botox can be used to reduce the intensity of the muscle post treatment and over time, the muscle may be retrained to a more physiological movement. Again, this is adjunctive therapy but is a nice option for patients that have had significant orthodontic relapse due to a hyperactive muscle.
BOTOX can also be used in patients as they get used to new dentures, especially with patients who have been edentulous for a long time and have old dentures and they are significantly overclosed. The dentures you make for patients may fit perfectly but with strong irregular muscle contractions, the patients will have a hard time getting used to their dentures and keeping in their mouths.
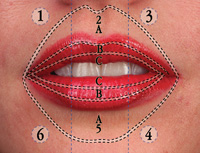
As people get older, the corners of the mouth begin to turn down. BOTOX can be placed in the depressor anguli oris muscles bilaterally to relax these muscles which will in turn raise the corners of the mouth. BOTOX can also be used to smooth the wrinkles around lips that are very commonly called smokers’ wrinkles. These wrinkles may not have anything to do with smoking, but have everything to do with the strong contractions of the orbicularis oris muscles.
SHOULD GENERAL DENTISTS ADMINISTER BOTOX THERAPY?
In the author’s opinion, there is a huge misconception and much confusion regarding the use of BOTOX therapy within the realm of dentistry by dentists. Right now, close to half the states in the United States and some provinces in Canada allow dentists to perform BOTOX procedures in all of the oral and maxillofacial areas. In other states, state dental associations are lobbying to allow dentists to begin performing these procedures. Certainly, as demonstrated in this article, the uses for BOTOX in dental treatment are within the scope of dental practice, as defined by most state dental boards. Readers are urged to become familiar with their state dental board laws regarding the definition of the scope of practice for dentistry in their locations.
With plastic surgeons, dermatologists, internal medicine physicians, obstetricians-gynecologists, opthamologists, podiatrists, nurses, physicians’ assistants, and medical aestheticians (who may not even be medically trained) delivering BOTOX to patients in the oral and maxillofacial areas, it is certainly time to recognize that dentists can be just as proficient in injections than any of these healthcare providers. Dentists also have much expertise in the oral and maxillofacial areas. We are also trained to be experts in the muscles of mastication and the muscles of facial expression which routinely receive these treatments.
Dentists are sometimes afraid that BOTOX and dermal fillers belong in medical arena and only physicians should perform these procedures. First of all, we are part of the medical arena and we are “real doctors.” Every time we inject local anaesthetic into a patient, we are delivering a medicinal agent into the body that has real potential for systemic complications. The only difference is that we have been trained to deliver local anaesthetic into the human body and are comfortable with dealing with the complications. (By the way, the adverse reactions and complications associated with the local anaesthetic we use are far more serious than those with BOTOX and dermal fillers.) After proper training, we can be equally comfortable with using BOTOX as in administering and managing the use of local anesthetics. Having now trained hundreds of dental professionals and other healthcare providers in BOTOX therapy, I can testify that dentists are the easiest to train, the most realistic and conservative with the treatment, and the best healthcare professionals to deal with any complications in the head and neck areas.
QUALIFICATIONS NEEDED
The other misconception that I run into routinely is that this takes a medical residency or months of training to learn how to perform BOTOX and dermal filler therapy for cosmetic and clinical uses. In terms of training, dentists often think that the other healthcare providers, such as plastic surgeons and dermatologists, go through extensive training in their residencies on BOTOX and dermal fillers.
I have spoken to, have worked with, and have trained physicians and nurses in BOTOX and dermal filler therapy. I have heard from numerous plastic surgeons, dermatologists, and general physicians that unless the residency has a cosmetic component, these topics are not even covered. Indeed, many dermatologists, and certainly most other physicians receive their training in BOTOX and dermal fillers through one- to 2-day courses. Nurses often receive on the job training. In many states, nurses and physicians assistants are allowed to deliver BOTOX, dermal fillers, sclerotherapy, laser and chemical peels, and mesotherapy in independent practices without a physician present.
Are we as dentists less qualified to deliver these procedures? In my opinion, we are among the best qualified to do so. We need to seriously rethink these issues as a profession and stop letting our politics get in the way of common sense as it relates to aesthetic facial procedures.
TRAINING IS THE KEY
Hands-on training is absolutely essential in learning how to provide these procedures and intertwining them with dental treatment plans. With proper training, dentists are usually more proficient than any of these other healthcare professions in providing these treatments to patients, both for dental and cosmetic needs. I have trained many dentists and other healthcare professionals and by far, dentists with their proficient knowledge of the facial anatomy and their experience with injections, are the best choice to provide these services to their patients and to realize the wonderful effects that BOTOX treatment can have on the smile lines and facial aesthetics.
CONCLUSION
It is time to broaden our horizons as a profession and use all of the tools available to us. BOTOX therapy is a conservative, minimally invasive treatment that can expand our therapeutic options for the benefit of our patients and is a natural progression of where we are going in the dental industry. These procedures are easy to accomplish by general dentists with proper training. Patients are motivated to accept these therapies and would be excited at having this done by their dentist, the healthcare professional of choice to deliver these procedures. This is the perfect complement and the next step in complete cosmetic dentistry.
References
- Naumann M, Albanese A, Heinen F, et al. Safety and efficacy of botulinum toxin type A following long-term use. Eur J Neurol. 2006;13(Suppl 4):35-40.
- Song PC, Schwartz J, Blitzer A. The emerging role of botulinum toxin in the treatment of temporomandibular disorders. Oral Dis. 2007; 13:253-260.
- Meunier FA, Schiavo G, Molgó J. Botulinum neurotoxins: from paralysis to recovery of functional neuromuscular transmission. J Physiol Paris. 2002;96:105-113.
- Borodic GE, Acquadro MA. The use of botulinum toxin for the treatment of chronic facial pain. J Pain. 2002;3:21-27.
- Kurtoglu C, Gur OH, Kurkcu M, Sertdemir Y, Guler-Uysal F, Uysal H. Effect of botulinum toxin-A in myofascial pain patients with or without functional disc displacement. J Oral Maxillofac Surg. 2008;66:1644-1651.
Dr. Malcmacher is a practicing general and aesthetic dentist in Bay Village, Ohio, and An evaluator for Clinicians Reports (formerly Clinical Research Associates), he has served as a spokesman for the Academy of General Dentistry and is a consultant to the Council on Dental Practice of the ADA. He is an international lecturer and author known for his comprehensive and entertaining style. His lecture schedule can be viewed at commonsensedentistry.com, where you can also find information about BOTOX and dermal filler training for dentists, teleconferences, audio CDs, and his free monthly e-newsletter. He can be reached via phone at (440) 892-1810 or via e-mail at dryowza@mail.com.
Disclosure: Dr. Malcmacher reports no conflict of interest.