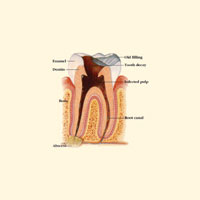
Take a look at Figures 1 and 2. They are stark reminders that despite our best efforts and planning, crowns will fail. Such failures may be due to patient carelessness with respect to unyielding foods (frozen candy bars, ice, etc), hidden ceramic defects stemming from faulty laboratory procedures, or, very commonly, inappropriate material selection for the crown itself. Whatever the reason, the patient presenting with a “recently” delivered crown in need of replacement has been a perplexing dilemma for most practitioners. Here are some commonly raised questions:
• How long has the crown been in service (certainly with respect to insurance carriers)?
• Did it break as a result of neglect or an accident?
• Must I replace this crown at no cost to the patient?
• If I charge a fee, how much is fair?
• Will my laboratory charge me for the remake?
• Even worse….how long can I nurse this thing along before I actually have to replace it?
 |
The circumstances under which this scenario usually plays out are awkward at best. The doctor often wants to play the good guy (perhaps out of guilt) and eat the cost of replacement while his or her stomach is turning, and the patient is looking to the doctor with hopeful, trusting eyes, and wants only to hear that replacement will be free. We’ve all been there. Why is this?
LEARN FROM THE RETAIL WORLD
Have you ever noticed that even low-cost consumer items come with extensive warranty documentation that states the manufacturer’s obligations to the consumer? Yes, we are quick to toss this out with the packaging, but if you take the time to read the warranty, you see that the manufacturer spells out what will take place in the event that the item fails to work properly.
Curiously, this approach has been neglected in dentistry (and medicine, for that matter). Call it professional “pride” if you will, but our dental brethren have often operated under the apologetic rule of “If it breaks, we’ll fix it…my bad, sorry…” If you think about it, however, there is scant logic in providing a $1,000 item (a crown) without having something in writing that states what will happen in the event of premature failure, for whatever reason.
Operating a 3-doctor general practice in central Connecticut that delivers a fair share of crown and bridge, my partner, Dr. Chris Boscarino, and I decided to provide patients with a written Service Policy at the time the crowns are scheduled; that is, before the procedure ever takes place.
THE LOGIC BEHIND THE POLICY
 |
| Figure 1. Crown failure. |
 |
|
Figure 2. Crown fracture. |
After playing with words for a bit, we decided to emulate a sort of “insurance policy,” whereby Dental Health Associates PC provides “coverage” on the crown, in a prorated sense, over a 5-year period, after which even insurance carriers deem the crown appropriate for replacement with a new crown. It was intended to appear as an act of “generosity” as opposed to one of “apology.” Our chief goal was to protect our practice from taking a financial hit when premature crown failures occurred, content simply to cover costs of replacement, if possible, rather than operate entirely in the red. Make no mistake, crown replacement at even a reduced cost is a no-win situation, but the opportunity to recover some of the replacement expense has to be a welcome one. And, if you are still doing business with the lab that made the crown, the lab bill will often be complimentary if the crown is replaced within a 5-year period. If not, you will likely include the new lab bill as one of the expenses that you seek to recover in the context of a crown Service Policy.
The other intangible provided by a pre-written policy is the good will that is hopefully generated as patients are made to understand that you are backing your restorative efforts in good faith.
Please understand that the agreement you see here is not written by an attorney and your patient may question it if, for instance, the crown failure occurs one week into the second year of service. Doctor discretion may be needed in borderline occurrences. At the very least, one has a starting point from which to operate. In most instances we’ve found that patients are comfortable with the policy. They are typically grateful not to have to pay in full to replace the crown. Yes, there will be an occasional patient who feels he or she shouldn’t have to pay anything. That patient can often be won over by reminding him or her of the policy provided when the crown was planned, and assuring the patient that you are merely seeking to cover the expense of replacement, not make a profit. Surprisingly, most patients can appreciate this.
Our Service Policy is presented on page 116. You may tweak it any way that suits you.
While the concept may appear foreign to our profession, the benefits as stated above are obvious. Having a predefined method for determining early failure replacement costs will soften the financial blow as well as create an orderly flow to handling this inevitably awkward moment that plagues us all. Needless to say, this type of policy can be extended to veneers, prosthetics, etc with the wording changed appropriately.
OPINION ONLY
While we’re on the subject, I will take this opportunity to share what experience has taught me with respect to significantly reducing the chances of indirect restorative fractures over the years. It’s really very simple.
Unless there is an extremely important reason not to, I choose porcelain-to-metal restorations for posterior full-crown restorations, including the bicuspids (some exceptions made on the first bicuspids for cosmetic reasons). Whether it is Captek or conventional PFM technologies featuring rigid, dependable substructures, their track record speaks for itself. I have personally been witness to far too many “all-ceramic” restorations placed in heavy impact areas that look beautiful at delivery but fail prematurely, usually catastrophically. Placing such restorations in those patients who brux adds insult to injury. Still, we are frequently beckoned to try new materials in search of the most natural look. They come and they go over the years, while the venerable PFM remains the modern day, dependable workhorse for our posterior restorative efforts. Please note that I refer specifically to posterior crowns in this instance, fully aware that more freedom exists when selecting materials to restore the anterior dentition. Suffice it to say that “newer is not always better,” and “buyer beware” aptly applies when prescribing your restorative choices.
CONCLUSION
Try as we might, even when everything is looking rosy, our restorative efforts can fail prematurely. We can reduce our exposure not only by making appropriate material selections, but also by having a policy in place for defraying the costs of replacement; reducing the red ink, as it were. Accept the included crown Service Policy as a gift from Dr. Chris Boscarino and myself. If you come up with some cool tweaks, we’d love to hear about them.
Dr. Goldstein practices general dentistry in Wolcott, Conn. He lectures and writes extensively concerning cosmetics and the integration of digital photography into the general practice. A regular contributing editor for Dentistry Today, he has also authored numerous articles for multiple dental periodicals both in the United States and abroad. He can be contacted at martyg924@cox.net or by calling (203) 879-4649. His current speaking schedule can be found at drgoldsteinspeaks.com or by visiting the Leaders in C.E. section of dentistrytoday.com.