
INTRODUCTION
Many patients present with both functional and aesthetic problems. The dentist must first listen to the concerns of the patient, then evaluate the clinical findings in order to correctly apply dental facial treatment planning principles. When appropriate, minimally invasive techniques using a multidisciplinary approach should be presented. This article shows the step-by-step thought process and treatment sequence for replacing and restoring a 20-year-old feldspathic minimal preparation veneer case. Verbal communication and clinical adjustments during each phase were critical to the successful outcome, including after the final cementation of the porcelain restorations. Collaboration with the patient invested her as an active participant in her aesthetic outcome and enhanced her satisfaction with both the process and the end result.
CASE REPORT
Diagnosis and Treatment Planning
A 45-year-old female patient presented with a chipped incisal edge of her tooth No. 7 veneer. She was unhappy with the bulkiness, color, and shape of her 20-year-old veneers. She remembered that her original dentist performed minimal preparation, and there was no composite temporization after tooth preparation while she was waiting for the veneers to be seated. She was concerned with the bulkiness and monochromatic appearance and was looking for a more natural and lifelike aesthetic result.
 |
 |
| Figure 1. Preoperative view: The incisal edges are hidden under the lower lip, and excessive gingival display is evident. | Figure 2. Note the uneven mandibular occlusal plane with crowding, incisal wear, and recession. |
 |
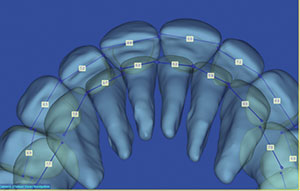
| Figure 3. The canines do not protect the front teeth in lateral excursion. |
She reported a history of mitral valve prolapse, and her physician stated that antibiotic premedication was not needed. Her yearly physical had been recently completed, stating that she was in good overall health.
A comprehensive dental exam was performed, which included a full-mouth series of radiographs, periodontal charting, and clinical photos. Evaluation of the photographs revealed that the edges of her maxillary incisors were hidden below her lower lip and she had excessive gingival display (Figure 1). The mandibular anterior region presented with mild crowding, incisal wear, rotations, recession, and previously placed Class V composites. The mandibular incisal plane was uneven, with the mandibular anterior segment (teeth Nos. 22 to 27) positioned 2.0 mm incisal to the posterior occlusal plane (Figure 2). The clinical evaluation also revealed a deep bite, with no canine protection of the anterior teeth in lateral excursions (Figure 3). She exhibited a parafunctional grinding habit in lateral excursion and protrusive, where she habitually ground on her canines and incisors. She presented with late clicking in both the right and left temporomandibular joints and a Class II Division I malocclusion.
A Kois deprogrammer was utilized to take a centric relation bite, and models were mounted. A functional analysis showed that the first point of contact in centric relation (CR) was the maxillary and mandibular right lateral incisors. This finding confirmed the diagnosis of a constricted chewing pattern.
The first step in dental facial treatment planning is evaluating the incisal edge and gingival position of the maxillary incisors (Figure 1). There are 4 ways to reposition the incisal edge: perio-restorative dentistry, orthodontics, orthognathic surgery, or a combination of both orthodontics and orthognathic surgery referred to as distraction osteogenesis. All options were discussed with the patient. If no orthodontic treatment was provided, the perio-restorative option of crown lengthening and subsequent tooth shortening would increase both the biomechanical and periodontal risk since significant tooth structure removal would be required and the crown-to-root ratio would become less favorable due to the removal of facial alveolar bone.
The patient agreed to an orthodontic consultation. The orthodontist recommended correcting the deep overbite, unconstricting the chewing envelope, and intruding the maxillary incisors in relation to her upper lip in repose (Figure 4). This treatment plan was accepted by the patient and would be implemented using SureSmile (Dentsply Sirona) lingual technology (suresmile.com) linked with CBCT digital design.
 |
| Figure 4. In this lateral cephalometric view, note that the central incisal edge position is tucked under the lip. |
SureSmile technology entails moving the teeth virtually (vertically and horizontally) and analyzing tooth mass and size from the maxilla, as compared to the mandible. All possible options can be seen on the computer, which minimizes errors in the mouth and shortens the overall treatment time. Preoperative evaluation reveals which arch needs recontouring or slenderizing, and which arch may be left with excess space. This case presented with excess tooth mass on the maxilla. The goal was to finish treatment with the ideal tooth size that would match the face, with minimal need for restorative intervention when the orthodontic treatment was completed. Due to previous symptoms, she was informed that her temporomandibular joint function would be monitored and that possible splint therapy could be necessary either during or after the orthodontic treatment.
Pre-Restorative Orthodontic Phase
As predicted, 6 months after the orthodontic phase was started, the orthodontist requested assistance with narrowing the anterior teeth via interproximal reduction (IPR) because they were too wide and bulbous in relation to her facial contours (Figure 5). The ideal length-to-width ratio of the central incisor has a range of 75% to 80%. At this time in treatment, the length was evaluated and left untouched because the teeth still required intrusion and the aligning of the gingival zeniths of teeth Nos. 6 to 11 (Figure 6).
On lingual evaluation, it was noted that porcelain was wrapped interproximally from the original reconstruction (Figure 7). When the IPR was done, every effort was made to remove only porcelain and conserve enamel in order to facilitate an additive and conservative approach to the post-ortho restorative reconstruction. The central incisors were slenderized by removing distal porcelain, using a diamond (#8850.31.016 [Brasseler USA]) (Figure 8).
The Golden Rule of Proportion in dentistry
states that the width of the lateral is 0.67 times the width of the central. The central width was measured and multiplied by 0.67. This calculated millimeter width was then used during the execution of the IPR step to obtain the final mesiodistal width of the lateral. Slenderizing of the interproximal of the laterals and canines occurred, followed by flattening of the anterior teeth. The facial surfaces were carefully recontoured to retain a thin layer of porcelain covering the tooth, which prevented darker tooth structure from showing through.
The orthodontist was instructed to finish the case with the incisors in as lingual and proclined a position as possible while still creating an idealized occlusion and chewing pattern. This would facilitate the preservation of tooth structure and allow the use of an additive protocol in the restorative phase. Additional intrusion using temporary anchoring devices (TADs) (Figure 9), the closing of spaces, rotation correction, and leveling of the occlusal plane occurred with respect to allowing room in the chewing pattern for porcelain on the lingual of the anterior teeth.
 |
 |
| Figure 5. A SureSmile overjet (Dentsply Sirona), showing excessive tooth width before interproximal reduction (IPR). | Figure 6. The calipers, measuring the adjusted width and depth. |
 |
 |
| Figure 7. Porcelain was present interproximally that was removed during IPR. | Figure 8. A frontal view of the left central incisor after distal IPR. |
 |
 |
| Figure 9. Temporary anchoring devices (TADs) were used to intrude the teeth to align gingival margins. | Figure 10. SureSmile treatment (after IPR and orthodontic movement), showing overjet reduction after IPR and set to a Class I molar and cuspid occlusion with a coincident midline. |
 |
 |
| Figure 11. Post-ortho: Note the ideal tooth and gingival display in the smile zone, ready for new veneers. | Figure 12. Ortho-facilitated, minimally invasive, enamel-based tooth preparation. |
After 24 months, the orthodontic treatment was completed when the correct tooth position with adequate occlusal space in the chewing cycle had been achieved (Figure 10). The patient was debanded, and Essix retainers were fabricated and delivered. Records were then taken for a digital diagnostic wax-up, and incisal, facial, and putty (Sil-Tech [Ivoclar Vivadent]) stints for the provisionals were fabricated.
The patient desired whiter mandibular teeth, so she was instructed to place whitening gel (Philips Zoom NightWhite [Philips Oral Healthcare]) inside the lower Essix retainer while she slept for 2 weeks (Figure 11).
Restorative Phase
The patient was appointed, and a composite shade selection for teeth Nos. 22 to 27 was accomplished by assessing the opacity and shade of the remaining tooth structure at the mandibular incisal edge.1 A shade A1B Body composite (Filtek Supreme Ultra [3M]) was chosen. A small increment was placed on the missing portion of tooth and light cured in order to preview and verify that a seamless, undetectable transition from tooth to restoration could occur with this shade. The incisal edges of teeth Nos. 22 to 27 were lightly beveled with a fine diamond to open up the enamel prisms (#850.31.016 [Brasseler USA]), then followed by micro-etching (MicroEtcher IIA [Danville Materials]). A total-etch technique was used, placing 37% phosphoric etch first on the enamel circumference and then on the dentin with a microbrush. After 15 seconds, the etchant was rinsed thoroughly with water, and then the tooth surfaces were lightly air dried (not desiccated), intentionally leaving a moist dentin surface. A single-bottle light-cured adhesive (ALL-BOND UNIVERSAL [BISCO Dental Products]) was applied and agitated for 20 seconds, air dried for 5 seconds, and then light cured for 10 seconds. A gold waxing instrument (Titanium 8A Instrument [Cosmedent]) was used to sculpt the composite. The verification of proper shape and form from a frontal perspective was accomplished, and, when the 3-D form was morphologically indistinguishable, the composite resin was fully light cured.
 |
 |
| Figure 13. Photographs of bis-acryl (Luxatemp [DMG America]) prototypes with shade tabs used to aid in selecting the final color. | Figure 14. When the porcelain case arrived in the office for delivery, a color verification process was carried out by placing the veneer on the composite dye (custom tab on the left) and checking the color against the shade tabs. |
 |
 |
| Figure 15. A1 and B1 shade tabs were used to evaluate the existing final color. | Figure 16. The removal of external stains, yielding a monochromatic B1 final shade. |
 |
 |
| Figure 17. Lightly dusting the restorations with an extra fine diamond in a sweeping motion to remove some of the external stain layer. | Figure 18. Postoperative 1 :1 view of HTBL 2 IPS e.max restorations with stains removed. |
Local anesthetic was administered on the maxillary arch. The Sil-Tech putty matrix would be used to create prototypes that the patient could preview. The prototypes, once approved and adjusted (if needed), would then also serve as a prep guide to ensure appropriate but minimal reduction. The putty stint was loaded with a shade A1 bis-acryl provisional material (Luxatemp [DMG America]) and seated over the maxillary arch. The patient previewed the resulting composite prototypes, and the shape and form were approved. She wanted a lighter final prototype than A1, so B1 was chosen to be used for the final set of provisionals.
Depth cuts were made over the composite prototypes using diamond burs (868D.31.030 [Brasseler USA]) across the gingival and middle third to establish the amount of facial reduction.2,3 Next, 2.0 mm was removed from the previously approved incisal edge length. A lingual chamfer design was chosen to enhance the resistance form of the preparation4 as well as to provide increased enamel surface area for increased bond strength. (The prepared teeth can be seen in Figure 12.)
The following records were taken and sent to the dental laboratory team: a Face-Bow (Panadent), maximum intercuspation position (MIP) bite registration (Futar Fast [Kettenbach LP]), vinyl polysiloxane (VPS) impressions (Honigum [DMG America]), provisional models, and detailed photo documentation. The lower teeth had a combination of both A1 and B1 shades, and, after the initial mock-up, the patient requested a lighter composite prototype. Provisionals were fabricated (shade B1 [Luxatemp]) by loading the provisional matrix with the bis-acryl material and seating it. The resulting provisionals were luted with a combination of spot etching and bonding using veneer cement (Duo-Link Universal [BISCO Dental Products]) in the center of the preparations and a temporary cement (TempoCem ID [DMG America]) at the peripheries. The patient was asked to drink coffee, tea, and red wine immediately following placement. The provisional would stain, leading to a shade shift of between one-half to one shade darker. The patient could then evaluate the color as it darkens, and, when the final color is chosen, the dentist can take a photo with a matching shade tab against the composite prototype and send it to the ceramist. This color is sealed by placing a glaze (LuxaGlaze [DMG]) over the provisionals and light curing for 20 seconds.
Two weeks later, the patient returned for an evaluation of the shape, form, color, and function of the provisionals, which she approved (Figure 13.) In order to achieve high-strength and aesthetic lithium disilicate restorations, IPS e.max Press Ingot HTBL 2 (Ivoclar Vivadent) was selected as the material of choice.5,6
When the porcelain case arrived in the office for delivery, a color verification process was carried out by placing the veneer on the composite dye and checking the color against the shade tabs (Figure 14). Then the IPS e.max restorations were placed intraorally for aesthetic evaluation (shape, color, and length) and approval by the patient. All 8 maxillary restorations were silanated (BIS-SILANE [BISCO Dental Products]), and the teeth were bonded (ALL-BOND UNIVERSAL) and luted into place using a light-cured resin cement (Variolink Esthetic LC [Ivoclar Vivadent]). Excess cement was then removed.
Next, an occlusal equilibration was done with the patient closing into MIP until all posterior teeth displayed bilateral and simultaneous forces. The functional occlusion was evaluated with the patient sitting up in the chair and chewing on thick (200 µm) horseshoe articulating paper (Bausch), which simulates the chewing envelope, activating the closing muscles. All functional adjustments were made by recontouring the composite on the mandibular dentition. Essix retainers were fabricated, and the patient was instructed to wear the Essix retainers indefinitely to maintain the achieved results.
A Post-Delivery Shade Challenge
Two weeks later, the patient returned and reported that she was unhappy with the color of her new veneers. She felt they were darker than her lower teeth. Photographs with B1 and A1 shade tabs (Figure 15) were taken with her veneers and lower teeth. The color prescription was reviewed, and the evaluation was confirmed that the veneer color was what had been previously requested. She had asked for natural-looking veneers that were imperceptible when compared to her existing dentition, which entailed color gradation and a combination of the A and B shades in the final porcelain. She agreed, but remained unsatisfied, still believing that the shade of the veneers was too dark.
Patients often ask for natural porcelain veneers but have worn monochromatic composite prototypes or, as in this case, monochromatic 20-year-old porcelain veneers. Patients may present with a chief concern that their existing veneers look “fake” and that they want something more natural and realistic looking. However, many patients, including this one, perceive the natural color gradation as dark and may dislike an “aesthetic natural” appearance. The presence of external staining on her veneers to mimic the natural appearance of her dentition was discussed with the patient.
It was jointly decided to decrease the saturation of color by removing some of the external stain. We agreed to remove all of the external stain from tooth No. 3 as a preview (Figure 16). A diamond (#8850.31.016 [Brasseler USA]) was used to remove the superficial stain, revealing monochromatic porcelain that presented as a B1 shade. She was instructed to go home and evaluate the color of the molar and see if she wanted to return later and have the stain removed from all of her maxillary porcelain veneers.
She returned one week later, electing to have the stain removed from the remaining veneers. An extra fine diamond (#133EF.31.01 [Brasseler USA]) was used with a sweeping motion, lightly dusting the surface throughout the entire facial of the anterior teeth (Figure 17). The goal was to lighten the veneers and maintain a degree of color gradation by removing some of the stain but leaving approximately 30% behind on the surface. After this, the veneers were polished to restore the surface luster (Jiffy Brush and Diamond Polishing Paste [Ultradent Products]). At the completion of these steps to adjust the shade, she was very happy (Figures 18 and 19).
 |
 |
| Figure 19. (a) Pre-op smile. (b) Post-op smile with the completed lithium disilicate veneer restorations (IPS e.max [Ivoclar Vivadent]). (Note the perfect alignment of the gingival zenith with the upper lip and the incisal edges with the lower lip.) |
Follow-Up Care
Wearing orthodontic brackets is similar to wearing a deprogrammer for 24 months. This patient may still posture her jaw forward and grind her teeth together, even after ortho and restorative phases have been completed. Maxillary and mandibular Essix retainers were fabricated, and the patient was instructed to wear both retainers indefinitely. The restorative plan included the monitoring of symptoms and to read the occlusal surfaces on the Essix retainers at her hygiene recare visits. If the retainers show occlusal marks or distortion and mutilation from nighttime grinding, a flat plane occlusal guard will then be fabricated.
CLOSING COMMENTS
It is paramoun
t when gathering all the data in the initial consultation that the dentist not only looks at the aesthetics but also recognizes and explains to the patient how the teeth function together.
This case teaches us how to restore aesthetics by setting the maxillary teeth correctly within the framework of the face and by addressing and correcting any functional problems so that the mandibular dentition functions in a proper relationship to the maxilla with less wear and a lower chance of failure of the restorations placed. This approach improves the longevity of the restorations and prognosis of the natural teeth.
Office systems that include patient-approval checkpoints throughout the procedures are important and necessary to have, along with buy-in from the patient. Even when using these checks and balances, patients may return (even many months later) with concerns and requests that necessitate changes. Just because the restorations are cemented does not necessarily mean that the case is completed. However, continuing to work and collaborate together can result in excellent patient satisfaction in the end.
Acknowledgments:
The concepts shown here are the teachings of the Kois Center and the American Academy of Cosmetic Dentistry (AACD). The author would like to thank Dr. Howard Henry, the treating orthodontist, Sandy Cooke for her beautiful ceramics and laboratory support, and Dr. Jean Martin, for her editing expertise.
References
- Bassett JL. Esthetics built to last: treatment of functional anomalies may need to precede esthetic corrections. Compend Contin Educ Dent. 2014;35:118-122.
- Gürel G. The Science and Art of Porcelain Laminate Veneers. Hanover Park, IL: Quintessence Publishing; 2003:241-251, 261-276.
- Magne P, Belser UC. Novel porcelain laminate preparation approach driven by a diagnostic mock-up. J Esthet Restor Dent. 2004;16:7-18.
- Chaiyabutr Y, Phillips KM, Ma PS, et al. Comparison of load-fatigue testing of ceramic veneers with two different preparation designs. Int J Prosthodont. 2009;22:573-575.
- Anusavice KJ. Standardizing failure, success, and survival decisions in clinical studies of ceramic and metal-ceramic fixed dental prostheses. Dent Mater. 2012;28:102-111.
- Bühler-Zemp P, Völkel T, Fischer K. Scientific Documentation IPS e.max Press. Schaan, Liechtenstein: Ivoclar Vivadent AG; 2011.
Dr. Bassett practices comprehensive restorative and aesthetic dentistry in Scottsdale, Ariz. She is an Accredited Fellow of the American Academy of Cosmetic Dentistry and served as president from 2015 to 2016. Dr. Bassett is a Kois clinical instructor, a member of the Academy of Fixed Prosthodontics, a Diplomate of the American Board of Aesthetic Dentistry, a Fellow in the AGD, an associate member of the American Academy of Esthetic Dentistry, and a member of the Catapult Education Speaker’s bureau. She can be reached via email at drmouthy@aol.com or via the website drbassett.com.
Disclosure: Dr. Bassett reports no disclosures.
Related Articles
Digital Design: Predictability, Profitability, and Efficiency
Foundation for a Successful Smile Makeover: Understanding Bleaching Choices and Techniques
AACD Reports Bigger Profits for Practices That Offer Cosmetic Procedures

