



One of the most challenging issues in implant dentistry is maintaining the hard tissues around the implant head so the soft tissue is supported in developing and sustaining natural gingival contours. This is the essence of the term “pink aesthetics.”
The critical determinant of this process is the abutment/implant connection. A stable connection with no development of a microgap during function will prevent bacterial infestation and colonization of that connection with subsequent endotoxin production, which is so deleterious to the peri-implant bone levels.
Although the internal hex reigns as the most predominant abutment/implant connection, it is not the most stable. I have been restoring dental implants for almost 25 years and had become accustomed to crestal bone loss down to the first thread.
 |
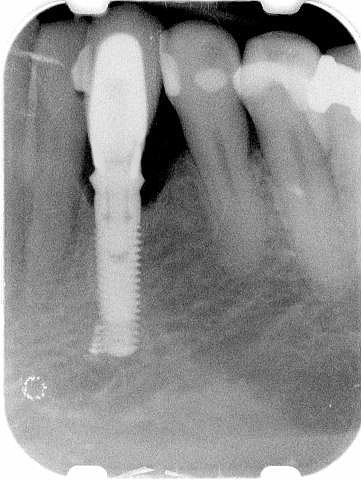 |
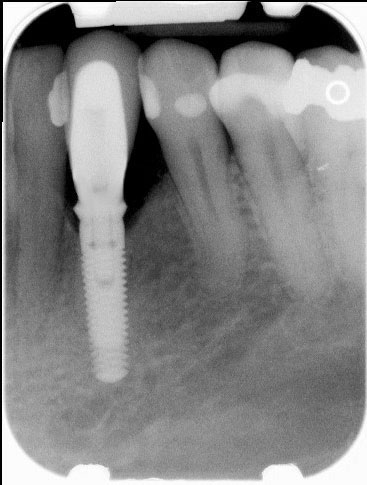
| Figure 1. A radiograph of an internal hex connection implant one week after restoration placed at the No. 22 position. | Figure 2. A 14-month post-restoration radiograph of that same implant exhibiting significant crestal bone loss about its head. |
Euphemistically termed “remodeling,” such bone loss is different than peri-implantitis only in degree and is why I have called the vast majority of these systems members of “The First Thread Club.”® This loss of hard-tissue scaffolding (Figures 1 and 2) has a direct effect on gingival architecture, producing less than successful results (Figures 3 and 4).
The tapered connection, especially the true Morse taper of 5.7° as featured in the Ankylos system from DENTSPLY implants, provides a much more stable abutment/implant interface. Used to attach jet engines to the wings of airliners, the Morse taper is among the most tried and true fixtures in the engineering world. It virtually eliminates any microgaps and provides a hermetic seal that prevents bacterial invasion of the abutment/implant juncture.
 |
 |
| Figure 3. A one-week post-restoration clinical photo of that same case. | Figure 4. Due to the bone loss seen radiographically, the marginal gingiva has grayed and a portion of the implant’s head is visible clinically 14 months later. |
 |
 |
| Figure 5. An 18-month post-restoration radiograph of a true Morse taper implant (Ankylos) at the No. 18 position showing bone growth over its shoulder impinging on the abutment. | Figure 6. A 36-month post-restoration radiograph of 2 implants 2.8 mm apart. Note that the crestal bone is up by their shoulders and nowhere near their first threads. |
 |
| Figure 7. A 36-month clinical photo of that case shows natural looking gingiva with fully developed interproximal papillae that are the definition of brilliant pink aesthetics in implant dentistry. |
The result of this stability is actual growth of bone over the shoulder of the implant (Figure 5) with this system along with preservation of bone levels between adjacent implants, even when they are less than 3 mm (Figures 6 and 7), that will uphold natural looking gingival profiles.
In the dental implant world of “pink and white aesthetics,” pink aesthetics almost totally depends on its primary hard-tissue platform. The true Morse taper connection, as opposed to the internal hex, maintains and fosters that platform to the point where pink aesthetic challenges are a thing of the past.
 Dr. Barry F. McArdle graduated from Tufts University School of Dental Medicine in 1985 and has been practicing general dentistry on the New Hampshire seacoast ever since. He has served on the active medical staff in dentistry of Concord Hospital in Concord, NH, and on the board of directors of Priority Dental Health, the New Hampshire Dental Society’s Direct Reimbursement entity. He is a co-founder of the Seacoast Esthetic Dentistry Association, which is headquartered in Portsmouth, NH. He is the founder of Seacoast Dental Seminars, also headquartered in Portsmouth. He has authored numerous other articles internationally in major peer-reviewed publications. He can be reached at (603) 430-1010, at drmcardle@seacoastdentalseminars.com, seda@dentalesthetics.com, or by visiting mcardledmd.com.
Dr. Barry F. McArdle graduated from Tufts University School of Dental Medicine in 1985 and has been practicing general dentistry on the New Hampshire seacoast ever since. He has served on the active medical staff in dentistry of Concord Hospital in Concord, NH, and on the board of directors of Priority Dental Health, the New Hampshire Dental Society’s Direct Reimbursement entity. He is a co-founder of the Seacoast Esthetic Dentistry Association, which is headquartered in Portsmouth, NH. He is the founder of Seacoast Dental Seminars, also headquartered in Portsmouth. He has authored numerous other articles internationally in major peer-reviewed publications. He can be reached at (603) 430-1010, at drmcardle@seacoastdentalseminars.com, seda@dentalesthetics.com, or by visiting mcardledmd.com.
Related Articles
The Immediate Smile: Fixed Provisionalization Using Digital Technology
Unique Attachment System for Implant-Supported Dentures
Co-Diagnosis in Smile Design: Involving Patients in the Ownership of Their Outcomes








