
INTRODUCTION
A consideration of available restorative space is critical when fabricating implant-supported overdentures.1,2 These prostheses are frequently involved in higher functional loading compared to conventional complete dentures, rendering them susceptible to fatigue degradation and fracture.3,4 A minimum denture base thickness for implant overdentures should be approximately 2.0 mm, and the minimum denture tooth height should be approximately 3.0 mm.2,5 A reduction in denture base dimensions to accept the attachment components render the prosthesis more susceptible to fracture.6 The incorporation of a metal framework has been recommended to maintain physiologically acceptable denture base contours and improve resistance to denture base fractures.6-9 This incorporation makes the prosthesis stronger compared to the use of acrylic resin alone. In addition, the prosthesis has greater resistance to fatigue and provides improved patient comfort.10,11
Another consideration in space management is the choice of overdenture attachment. LOCATOR attachments (Zest Dental Solutions) possess optimal vertical and horizontal height, making them a desirable choice when there is insufficient restorative space.2 In addition to its low-profile design, pivoting technology, durability, and ease of-use have made the LOCATOR attachment a preferred choice for retaining tissue-supported, implant-retained overdentures.12-16 The next-generation LOCATOR abutment (LOCATOR R-Tx abutment [Zest Dental Solutions]) permits a 50% increase in pivoting capability, potentially reducing the amount of load applied to the implants.17 This improvement in pivoting capability also helps decrease the wear/damage of the retention inserts when the implants are divergent (up to 60°). The pink anodization of the LOCATOR R-Tx denture attachment housings (DAHs) improves aesthetics by reducing the amount of metallic colors showing through the acrylic resin denture base.17 The LOCATOR R-Tx removable attachment system is designed to be stronger and simpler than the traditional LOCATOR abutment (Zest Dental Solutions), but it relies on the same restorative techniques as the conventional LOCATOR.18,19
The purpose of this clinical article is to describe the steps to be used in rehabilitating a patient with inadequate restorative space using implant-supported overdentures with various means of prosthetic accommodation.
CASE REPORT
Diagnosis and Treatment Planning
A 67-year-old, Caucasian, female patient presented with the chief complaints of poor aesthetics and low self-esteem, along with pain, discomfort, and a bad mouth odor. She was very anxious and indicated that she wanted quick treatment with a minimum number of invasive procedures. A comprehensive assessment was performed, including a detailed intra- and extraoral examination and a complete mouth series of radiographs (Figure 1). The diagnostic procedures revealed that the remaining natural teeth (Nos. 6 to 12, 14, 22 to 25, 27, 30, and 31) could not be retained due to extensive caries, periodontal disease, and/or endodontic infections and would need to be extracted.
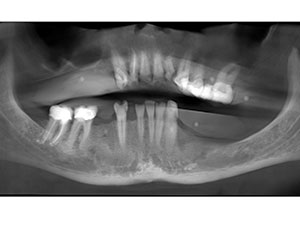 |
| Figure 1. Panoramic radiograph of the patient. |
Diagnostic impressions were made for both arches. Casts were generated and mounted on a semi-adjustable articulator using interocclusal records and a face-bow transfer. Mounted casts with clinically adjusted wax rims were used to measure available vertical restorative space for both arches, which was found to be inadequate.1,2 Maxillary and mandibular cameogram impressions were made using a rigid-viscosity, quick-polymerizing vinyl polysiloxane (VPS) impression material (Flexitime Monophase Pro Scan [Kulzer]) to identify spatial boundaries (horizontal restorative space) for the arches and relate this information to the design of the prostheses.20 The lips were retracted bilaterally, and the impression material was injected under the lip, extending from the left posterior vestibule to the right posterior vestibule and covering the dentition. The retractors were removed, and the patient was asked to pucker her lips outward, swallow, and smile forcibly to create a functional record.21 She was asked to perform these movements repeatedly until the impression material polymerized. Upon completion, the cameogram impression was removed from the mouth and inspected. A VPS putty index (Flexitime Easy Putty [Kulzer]) was fabricated to surround the cameogram and oriented to an indexed position on the master cast.22 The space between the index and the natural teeth indicated that additional labial/buccal restorative space was available for the maxillary prosthesis, which would permit labial positioning of the prosthetic teeth and the denture base. Additional labial/buccal restorative space was not available for the mandibular prosthesis.
 |
 |
| Figure 2. Radiographic markers incorporated in the maxillary cameogram. | Figure 3. Radiographic markers were incorporated in the mandibular cameogram. |
 |
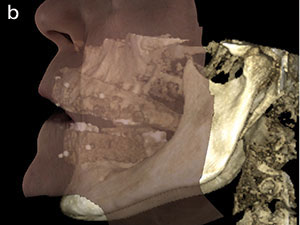 |
| Figure 4. A CBCT scan (Dentri [HDX WILL NORTH AMERICA]) of the patient with the cameogram placed in the patient’s mouth. (a) Frontal view; (b) profile view. |
Radiographic markers were incorporated in the maxillary and mandibular cameograms (Figures 2 and 3) above the location of the teeth and on their gingival surfaces and the dual cone beam computed tomography (CBCT) scans (Dentri [HDX WILL NORTH AMERICA]) obtained. One scan was made of the patient with the cameogram placed in the patient’s mouth (Figure 4), and another scan was made of the cast with the cameogram appropriately positioned on it. The raw data obtained from the scans was then converted to digital imaging and communications in medicine (DICOM) data, merged, and used for evaluating and planning optimal implant positions and angulations. The patient was given various treatment options for full-mouth rehabilitation (following the extraction of natural teeth), including implant-supported overdentures, fixed complete dentures, metal-ceramic/zirconia fixed restorations, and complete dentures. The patient chose maxillary and mandibular implant-supported overdentures for restoring her maxillary and mandibular arches. Alveoloplasty was indicated for both ar
ches to gain vertical and horizontal restorative space.
Clinical and Laboratory Protocols
After obtaining patient consent, the maxillary and mandibular mounted casts, maxillary cameogram, and putty index were sent to the laboratory along with detailed instructions for the fabrication of immediate transitional prostheses. The patient was referred to a surgeon for extraction of the remaining natural teeth and alveoloplasty. The remaining natural teeth were extracted, and the sockets were filed with a bone graft material (Symbios [Dentsply Sirona]). Alveoloplasty was minimally performed in both the arches due to anatomic limitations. Hence, the immediate transitional dentures had to be thinned out (especially the mandibular denture) to fit the oral tissues appropriately (Figures 5 and 6). The transitional dentures were relined with a soft material (PermaSoft [Dentsply Sirona]) and placed in the patient’s mouth. The occlusal vertical dimension (OVD) was intentionally increased by 3.0 mm via the addition of a thick lining material. If the patient would be able to adapt and/or accommodate this change, this increase in OVD would aid in gaining restorative space at the time of fabrication of the definitive restorations. At the time of placement, the patient felt that the teeth were too big for her; however, she was very pleased with the aesthetics. She was informed that it would take a period of time to accommodate. The patient was recalled regularly for evaluation and maintenance. At the 3-week recall appointment, she stated that she was very comfortable with the prostheses.
 |
 |
| Figure 5. The thin maxillary immediate prosthesis. | Figure 6. The mandibular immediate prosthesis. |
The tissues were allowed to heal for 3 months. Relined maxillary and mandibular immediate dentures were duplicated, radiographic markers were incorporated in the duplicate dentures, and dual CBCT scans were obtained. The raw data obtained from the scans was then converted to DICOM data and used for planning optimal implant positions and angulations for the definitive implant-supported overdentures. Implants were planned in the locations of teeth Nos. 6, 8, 10, 12, 22, 24, 26, and 30 on the CBCT implant planning software (Anatomage). The maxillary implants were planned with a labial inclination within the confines of the maxillary prosthesis. Apical placement of the implants by 2.0 to 3.0 mm to gain vertical restorative space was not a viable option due to anatomic limitations.
A 3-D, stereolithic surgical guide was acquired for the patient using the data generated during implant planning (Anatomage Guide [Anatomage]). The surgical guide was placed in the mouth and fixated. The implants were placed with a flapless procedure using the surgical guide (Astra Tech EV implants [Dentsply Sirona]). Healing abutments were also placed. The old reline material was removed from the transitional prostheses, and they were relined again with a soft reline material (PermaSoft). The patient was recalled at 24 hours and then at 2 and 4 weeks for evaluation and maintenance. She was asked to return after 3 months for the fabrication of the definitive prostheses.
 |
 |
 |
 |
| Figure 7. The registration of interocclusal records using printed record bases and an intraoral jaw recorder. |
 |
| Figure 8. Registration of the neutral zone record. |
Fabrication of Definitive Restorations
The implants were allowed to heal for 4 months. The patient presented with good tissue health and with no apparent trauma caused by the transitional denture. Primary impressions, definitive impressions, the maxillo-mandibular jaw relationship (Figure 7), and neutral zone records (Figure 8) were completed. The patient was able to adjust to the increase in OVD in the transitional dentures, which aided in gaining mandibular vertical restorative space. Wax trial placement procedures were completed. LOCATOR attachments were planned to retain and support the overdentures due to their low vertical and horizontal profiles. However, due to the configuration of bone and labial inclination in the maxilla, the implants could not be placed parallel to each other. There was a divergence of 40° between the implants. Newly introduced LOCATOR abutments (LOCATOR R-Tx), which may be used with an implant divergence of up to 60°, were used as attachments for the overdentures. All the records and casts, the LOCATOR R-Tx abutment assembly, and detailed instructions were sent to the laboratory. The lack of horizontal mandibular restorative space necessitated the incorporation of 2 lingual protuberances in the mandibular definitive prosthesis to accommodate the retentive housings. To improve patient comfort, strength and fracture resistance of the prostheses’ metal frameworks were planned for the patient. The frameworks were tried in the patient’s mouth, adjusted as necessary, and sent back to the laboratory to be incorporated in the design of the definitive maxillary (with an open palate design) and mandibular overdentures (Figures 9 and 10).
 |
 |
| Figure 9. The definitive maxillary denture. |
 |
 |
 |
| Figure 10. The definitive mandibular denture. |
The prostheses were trial placed, and their fit and occlusion were evaluated and adjusted. The LOCATOR R-Tx abutments (retrieved from the laboratory) were carefully attached to the implants and torqued as per the manufacturer specifications (Figures 11 and 12). The DAHs (also retrieved from the laboratory) were seated over the abutments. The prostheses were trial placed in the patient’s mouth to reverify the fit and occlusion, as well as to ensure that there was no contact of the DAH with the recesses created in the prostheses (Figures 13 and 14). The recesses were roughened and subjected to airborne particle abrasion using 50-μm aluminous oxide, and the DAHs were cleaned and dried. A metal-bonding acrylic agent (U bar metal bonding cold cure [Protech]) was applied to the recesses, and the DAHs were picked up directly by utilizing a chemically polymerizing resin material (CHAIRSIDE Attachment Processing Material [Zest Dental Solutions]) as per the manufacturer recommendations (Figure 15). The prostheses were adjusted, finished, and polished as needed. The black processing inserts were removed and replaced with blue and gray retention inserts using the LOCATOR R-Tx tool (Figure 16). The prostheses were finished, polished, and placed in the patient’s mouth (Figure 17). The patient was given oral hygiene demonstrations and provided with the cleaning aids necessary to maintain hygiene of the prostheses and the oral cavity, including the locator abutments. She was also given a printed copy of detailed home care instructions and placed on a biannual recall schedule. At the recall appointments, she stated that she was very comfortable and pleased with the retention, stability, and aesthetics of the definitive prostheses (Figure 18).
 |
 |
| Figure 11. LOCATOR R-Tx abutments (Zest Dental Solutions) attached to maxillary implants. | Figure 12. LOCATOR R-Tx abutments attached to mandibular implants. |
 |
 |
| Figure 13. Recesses created in the maxillary prosthesis. | Figure 14. Recesses created in the mandibular prosthesis. |
 |
 |
| Figure 15. Denture attachment housings were picked up in the mandibular denture. | Figure 16. Black inserts were replaced with blue and gray retention inserts in the maxillary prosthesis. |
 |
 |
| Figure 17. The definitive prostheses placed in the patient’s mouth. | Figure 18. The patient’s smile with the definitive prostheses. |
IN SUMMARY
Labial orientation of the maxillary prosthetic teeth and the denture base, an increase in OVD, the incorporation of metal frameworks, and the use of LOCATOR R-Tx attachments aided in accommodating the limited restorative space in this patient, permitting rehabilitation with implant-supported overdentures.
References
- Ahuja S, Cagna DR. Defining available restorative space for implant overdentures. J Prosthet Dent. 2010;104:133-136.
- Ahuja S, Cagna DR. Classification and management of restorative space in edentulous implant overdenture patients. J Prosthet Dent. 2011;105:332-337.
- Bakke M, Holm B, Gotfredsen K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: a prospective 5-year study. Int J Prosthodont. 2002;15:575-581.
- Pera P, Bassi F, Schierano G, et al. Implant anchored complete mandibular denture: evaluation of masticatory efficiency, oral function and degree of satisfaction. J Oral Rehabil. 1998;25:462-467.
- Alsiyabi AS, Felton DA, Cooper LF. The role of abutment-attachment selection in resolving inadequate interarch distance: a clinical report. J Prosthodont. 2005;14:184-190.
- Ahuja S, Jain V, Cagna D, et al. Fabricating a mandibular implant supported overdenture with a suspended framework. J Indian Prosthodont Soc. 2013;13:132-136.
- Rodrigues AH. Metal reinforcement for implant-supported mandibular overdentures. J Prosthet Dent. 2000;83:511-513.
- Cavallaro JS Jr, Tarnow DP. Unsplinted implants retaining maxillary overdentures with partial palatal coverage: report of 5 consecutive cases. Int J Oral Maxillofac Implants. 2007;22:808-814.
- Sadowsky SJ. Treatment considerations for maxillary implant overdentures: a systematic review. J Prosthet Dent. 2007;97:340-348.
- el Ghazali S, Glantz PO, Strandman E, et al. On the clinical deformation of maxillary complete dentures. Influence of denture-base design and shape of denture-bearing tissue. Acta Odontol Scand. 1989;47:69-76.
- Rueggeberg FA. Dental materials for complete dentures. In: Rahn AO, Ivanhoe JR, Plummer KD, eds. Textbook of Complete Dentures. 6th ed. Shelton, CT: People’s Medical Publishing House; 2009:10.
- Evtimovska E, Masri R, Driscoll CF, et al. The change in retentive values of locator attachments and Hader clips over time. J Prosthodont. 2009;18:479-483.
- Büttel AE, Bühler NM, Marinello CP. Locator or ball attachment: a guide for clinical decision making [in French, German]. Schweiz Monatsschr Zahnmed. 2009;119:901-918.
- Trakas T, Michalakis K, Kang K, et al. Attachment systems for implant retained overdentures: a literature review. Implant Dent. 2006;15:24-34.
- Chikunov I, Doan P, Vahidi F. Implant-retained partial overdenture with resilient attachments. J Prosthodont. 2008;17:141-148.
- Kleis WK, Kämmerer PW, Hartmann S, et al. A comparison of three different attachment systems for mandibular two-implant overdentures: one-year report. Clin Implant Dent Relat Res. 2010;12:209-218.
- Baba NZ, Al-Harbi FA, AlRumaih HS, et al. A novel extended range attachment system to retain implant overdentures: a clinical report. J Prosthodont. 2019;28:3-9.
- Goodacre CJ, Bernal G, Rungcharassaeng K, et al. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90:121-132.
- Pastor H. Titanium-carbonitride-based hard alloy for cutting tools. Mater S
ci Eng A. 1988;105-106:401-409. - Massad JJ, Wong D, Wicks RA, et al. Prospectively engineered implant placement. Dent Today. 2017;36:110-116.
- Massad JJ, Cagna DR, Wicks RA, et al. Cameograms: a new technique for prosthodontic applications. Dent Today. 2016;35:80-85.
- McDonald GT, Larsen HD. Laboratory procedures for the neutral zone denture technique. Quintessence Dent Technol. 1985;9:287-290.
Dr. Massad is an associate professor in the department of graduate prosthodontics at the University of Tennessee Health Science Center (UTHSC) College of Dentistry in Memphis; an associate faculty at the Tufts University School of Dental Medicine in Boston; an adjunct associate faculty of the department of comprehensive dentistry at the University of Texas Health Science Center at San Antonio (UT Health San Antonio) School of Dentistry; and an adjunct professor in the department of restorative dentistry at Loma Linda University in Loma Linda, Calif. He has a private practice in Tulsa. He can be reached at joe@joemassad.com.
Dr. Ahuja is an adjunct assistant professor in the department of prosthodontics at the UTHSC College of Dentistry. She is a consultant for several dental clinics in Mumbai, India, and also for Lutheran Medical Center in New York City. She has lectured nationally and internationally on various prosthodontic topics. She has been published in multiple peer-reviewed national and international journals and is the coauthor of the textbook Applications of the Neutral Zone in Prosthodontics. She can be reached at sahuja@uthsc.edu.
Dr. Wicks is a professor in and chairman of the department of prosthodontics at the UTHSC College of Dentistry, where he received his DDS degree in 1978. He was in private practice from 1979 to 1990. After receiving his MS degree and certificate in the specialty of prosthodontics from the UT Health San Antonio School of Dentistry in 1993, he conducted prosthodontic research and directed the undergraduate curriculum in removable prosthodontics and dental implants at the UTHSC College of Dentistry. He can be reached at rwicks@uthsc.edu.
Dr. Goodacre received his DDS degree from Loma Linda University and an MSD degree in prosthodontics and dental materials from Indiana University. He served as the chair of prosthodontics at Indiana University and dean of the Loma Linda University School of Dentistry. He is a Diplomate and past president of the American Board of Prosthodontics and past president of the American College of Prosthodontists and the Academy of Prosthodontics. He is a member of the board of directors of the Foundation for Oral Rehabilitation and chairs its education council. He has published more than 220 articles, abstracts, textbooks, and textbook chapters. In addition, he has developed or helped develop 17 online CE courses, 11 electronic education programs, and 3 eBooks. He currently holds the title of distinguished professor at Loma Linda University and teaches in its Advanced Education Program in Implant Dentistry. Dr. Goodacre maintains a private prosthodontic practice. He can be reached at cgoodacre@llu.edu.
Disclosure: The authors report no disclosures.
Related Articles
The Next Generation Attachment System
Implant Overdentures: Selections for Attachment Systems

