


INTRODUCTION
Let’s face it. Most of us have had some exposure to the TMJ in dental school, but it was just too complicated or too abstract that we just didn’t pay attention. How can this joint so far away from the teeth affect our dental work? We focused on the details and the techniques of cavity and crown prep, did the lab work necessary for our prosthodontics courses, and paid lip service to the diagnostic sciences. But where did this TMJ thing fit in? If a TMD condition arises, we were taught to fabricate splints and send the patient off to an oral surgeon or orofacial pain specialist, and, for the majority of us, that was about it.
Imagine this scenario, which is an amalgamation (no pun intended) of multiple true stories. You have spent the past 9 to 18 months perfecting your full-mouth reconstruction/orthodontic plus or minus orthognathic surgery/All-on-4/implant-supported prosthesis for your patient. Your patient is particularly difficult to deal with, and, after multiple adjustments and many months and dollars later, you have what you think is the perfect outcome, and the patient walks out of your clinic happy until a few months or years later, when he or she comes back complaining that his or her front teeth don’t touch anymore. You look in the mouth, and, lo and behold, there is a gap between the upper and lower anterior teeth, and you can find nothing in the mouth that could possibly have caused it. You could have sworn you had even contacts all around when you finished your work. Now, a few teeth are conspicuously bare of articulating paper markings, and the patient is complaining that his or her bite does not feel right or that his or her teeth don’t look good. This is a frustrating position for dentists to find themselves in, especially after extensive and tedious dental work and/or surgery, but it is a situation that can occur if the TMJ condition and orthopedic stability of the TMJ and occlusion are not assessed prior to treatment planning and execution.
While it is impossible to comprehensively review every single type of bite change and every TMJ condition leading to this kind of change in this article, the basic understanding of this process is the knowledge that the TMJ condyle is connected to the mandible…which houses the mandibular teeth…which articulate with the maxillary teeth…which are housed in the maxilla…which is connected to the palatine bone…which is connected to the sphenoid bone…which is connected to the temporal bone…which contacts the other half of the TMJ, the glenoid fossa. This aforementioned relationship sounds like a variation of the popular children’s song “Dem Bones.” Still, the connectedness of the human body in this fashion is really something that slips under the radar in many dental school programs. In summary, your upper jaw and lower jaw articulate in 2 places (if one was to consider the entire cranium an extension of the upper jaw)—the TMJs and the teeth—and structural and positional changes in one of these articulations can affect the other.
DISCUSSION
The orthopedic stability of a joint means that it is in a centered and reproducible position in which it functions optimally. The head of the humerus or the femur needs to be in an orthopedically stable situation to function to the best of its ability and range of motion without ligament or muscle strain. In the TMJ, the situation is a little different because we have 2 points of articulation between the cranium and the mandible: the 2 TMJs and the upper and lower dentitions. The orthopedically stable condition is when the teeth are in maximum intercuspation (what some circles call “centric occlusion [CO]”), and the condyles are seated in the fossa (what the same circles call “centric relation [CR]”). If the teeth are together and the condyles are not seated, then this is an orthopedically unstable occlusion (what those same circles call “CR-CO shift or discrepancy”). The terminology and the concepts are ever-evolving, but the principle is the same: If you want your final dental or prosthetic occlusion to be stable, you need to diagnose and respect the TMJ condition and position and understand the role of that joint and its dysfunction in the emergence of bite changes.
One orthopedically unstable occlusion is called “dual bite formation,” which is technically a CR-CO discrepancy, as it has been called in the past. It can form as a result of an acquired anterior position of the mandible. This anterior position can be due to auto-advancement or iatrogenic factors, which draw the condyles down and forward (Figure 1). Patients can auto-advance and hold their mandibles forward for various reasons, such as vanity because of a recessive and unattractive mandible, bringing a Class II mandible into function, or an attempt to increase airway dimensions by drawing the tongue and floor of the mouth forward through the attachment of these muscles to the mandible. Some dental treatments, such as orthodontic appliances and sleep appliances, can also advance the mandible. If the occlusion is altered in this forward position, or if the teeth super-erupt and come into occlusion in this forward mandibular position, the condyles will remain down and forward despite the teeth occluding fully. With time and relaxation of the muscles of mastication, the condyles will seek orthopedic stability (ie, they will seat gradually into the fossa), and as the condyle creeps back into the fossa, the mandible rotates back around a second molar tooth fulcrum and opens up the bite anteriorly (Figure 2). There are many patients who present to us as clinicians with teeth that seem to fit well but, in reality, have a condylar position that is not orthopedically stable, and it is our job to diagnose these prior to altering the occlusion or restoring it extensively because if the TMJ foundation is not stable, the dental house that we are building will not be stable.

Figure 1. When teeth are in maximum intercuspation (MIP), the condyles should be seated in the fossae. These images show condyles in 2 separate patients that are (a) inferiorly and forward and (b and c) inferiorly positioned in the fossae with teeth in MIP; thus, the suspicion of orthopedic instability arises and should be confirmed clinically.

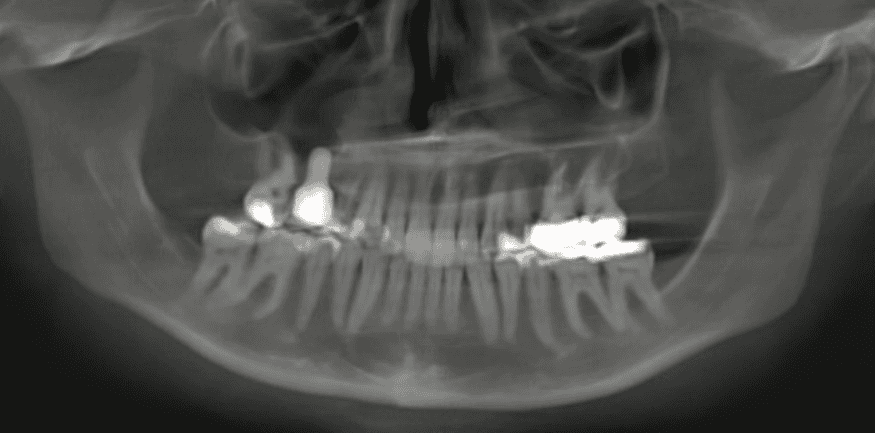
Figure 2. (a to d) The anterior open bite seen here is due to a dual bite relapse. The condyles are normal in height and morphology (d) with the posterior height of contour being lower than the anterior height of contours (compare to red arrows on Figure 6a). This morphology differentiates a dual bite relapse open bite from one caused by bilateral condylar height loss, where the height of contours can be at the same level (see Figures 4c, 5c and 6b).
Another orthopedically unstable situation occurs with structural and volumetric changes to the condyles, such as in the case of degenerative joint disease (osteoarthritis). Anything that reduces the height of the condyles will generate a space between the condyle and the fossa, and this extra space constitutes an orthopedically unstable situation. The condyles will gradually seat into the fossa and create that same phenotype of posterior rotation of the mandible and opening of the bite anteriorly. Patients can present to us with teeth that seem to fit well but may have degenerated condyles that are not completely seated in the fossae (Figure 3). The condylar height loss may have occurred before your treatment and the unseated condyles may not have been diagnosed prior to commencing work, or the degeneration may have occurred after your treatment. When we understand that degenerative joint disease is a biomechanical breakdown of the hard tissues that is preceded by the biomechanical breakdown of the soft tissues (internal derangement and disc displacement), it becomes clear that it is important to diagnose potentially vulnerable joints with disc displacements prior to starting treatment to inform the patient of the presence of this pre-existing condition that may compromise the stability of the treatment outcomes. In a few words, a clicking and popping joint is not normal. It is a biomechanically compromised joint that needs to be approached with care and diagnosed properly prior to starting dental treatment because a disc displacement is part of a continuum of articular tissue breakdown that may lead to jaw position changes and subsequent bite changes.

Figure 3. This patient’s condyles are undergoing active degeneration, resulting in loss in condylar height and increased joint space, creating an orthopedically unstable situation. Although the teeth are together now, this is an open bite waiting to happen.

Figure 4. (a) Bilateral end-stage degenerative joint disease with condylar height reduction and seating in the fossae has resulted in (b) the posterior rotation of the mandible and (b and c) the anterior open bite.
Anterior open bites are just one of the bite changes that can occur as a result of orthopedic instability of the condyles. When the TMJ condition and position change and consequent seating of the condyles occur bilaterally and synchronously, we can expect an even posterior rotation of the mandible and opening of the bite anteriorly (Figure 4). But there are variations of this orthopedic instability that can create different presentations of the open bite. If the culprit TMJ condition is unilateral, one can expect a subsequent rotation of the mandible in the coronal plane to seat the smaller condyle. This leads to the opening of the posterior bite on the contralateral side. If left unattended, the predicted teeth supereruption will occur, resulting in an occlusal cant with the affected side being more elevated (Figure 5). These conditions can also be asynchronous, where one TMJ undergoes these changes, resulting in the aforementioned outcomes, and then the other TMJ undergoes similar changes, resulting in the posterior rotation of the mandible and opening of the bite anteriorly. Thus, it is important to identify potentially vulnerable TMJs prior to commencing dental treatment to avoid adjusting or redoing the work and causing frustration for the dentist and the patient.

Figure 5. Unilateral condylar height loss due to end-stage degenerative joint disease has resulted in (a) seating of the condyle and (b to d) subsequent changes in mandibular symmetry and (c and d) occlusal canting (b), with the right side (affected side) being more elevated.

Figure 6. (a) A normal condyle morphology has a posterior height of contour that is lower than the anterior height of con- tour and a gradual forward bend of the condyle. (b) A condyle that has undergone degeneration and remodeling is smaller, has a flattened articular surface, and has a height of contour that can be at the same level as each other.
The assessment of orthopedic stability is mainly a clinical one, with multiple philosophies teaching different ways of diagnosing and treating it. As a radiologist, when examining a patient’s CBCT scan with teeth in maximum intercuspation (which is what I recommended), if his or her condyles are normal in morphology but their position is down and forward, then I suspect orthopedic instability typical of dual bite formation (Figure 1). If the condylar morphology is altered and they are not seated, then I suspect orthopedic instability as a result of condylar height loss (Figure 3). The key is the examination of the heights of contour of the condyles (Figure 6). In a normal condyle, the posterior height of contour should be lower than the anterior height of contour with a gradual forward bending of the condyle (Figure 6a). The end-stage remodeling result of degenerative changes is an alteration of the morphology of the condyle, with flattening of the articular surface and the heights of contours ending up nearly at the same level (Figure 6b). If there is an anterior open bite on the scan, I quickly look at the condyles to see if the condylar morphology is normal or degenerated to give the etiology of the bite change. I also note if there is still more potential for occlusal changes (ie, still more space potential for the condyles to seat further), which need to be verified clinically.
CONCLUSION
Of course, there are multiple other etiologies for bite changes that are more clinical diagnoses (such as digit sucking or tongue thrusting) or more complex diagnostic processes than I have space to describe here. The bottom line is this: If you do not diagnose your patients’ craniofacial conditions fully, you do not treat them fully and may run into issues with the stability of your treatments in the future. When you bring an oral and maxillofacial radiologist onto your dental team to help you diagnose your patient’s condition using his or her CBCT scans, we (the radiologists) will do what we can to help you (the clinicians) get to the bottom of the mystery of the changing bite.
ABOUT THE AUTHOR
Dr. Tamimi is the author of Specialty Imaging: Temporomandibular Joint and Sleep-Disordered Breathing and is a world-renowned speaker on the subject of oral and maxillofacial radiology. She runs her private practice in Orlando. She can be reached via her website at inspire-imaging.com or via email at info@inspire-imaging.com.
Disclosure: Dr. Tamimi reports no disclosures.








